Neonatal mortality remains a significant public health concern in Bangladesh, with a considerable number of newborns succumbing to preventable causes within the first 28 days of life. The common causes of neonatal death in the country are multifaceted, primarily stemming from preterm birth complications, severe infections such as sepsis and pneumonia, and birth asphyxia. Additionally, factors like low birth weight, lack of access to skilled birth attendants, inadequate postnatal care, and poor maternal health contribute to the high mortality rates. Socioeconomic disparities, limited healthcare infrastructure in rural areas, and insufficient awareness about newborn care further exacerbate the situation, highlighting the urgent need for targeted interventions and strengthened healthcare systems to address these preventable tragedies.
| Characteristics | Values |
|---|---|
| Preterm Birth Complications | Leading cause, accounting for ~30% of neonatal deaths (2021 data) |
| Neonatal Infections | Major contributor, including sepsis, pneumonia, and meningitis |
| Asphyxia (Birth Asphyxia) | Significant cause, often due to complications during labor and delivery |
| Low Birth Weight | Strongly associated with increased risk of neonatal mortality |
| Diarrheal Diseases | Contributes to dehydration and malnutrition in newborns |
| Congenital Anomalies | Responsible for a notable proportion of neonatal deaths |
| Lack of Access to Healthcare | Delayed or inadequate care exacerbates neonatal mortality rates |
| Maternal Malnutrition | Indirectly increases risk of low birth weight and preterm births |
| Poor Hygiene Practices | Increases susceptibility to infections in newborns |
| Delayed Breastfeeding Initiation | Linked to higher risk of infections and malnutrition |
Explore related products






What You'll Learn
- Prematurity and low birth weight: Leading cause due to inadequate prenatal care and maternal malnutrition
- Neonatal infections: Sepsis, pneumonia, and meningitis contribute significantly to mortality rates
- Birth asphyxia: Oxygen deprivation during delivery remains a critical factor in neonatal deaths
- Lack of skilled birth attendants: Limited access to trained healthcare providers increases risks during childbirth
- Poor healthcare infrastructure: Inadequate facilities and resources hinder timely and effective neonatal care
![]()
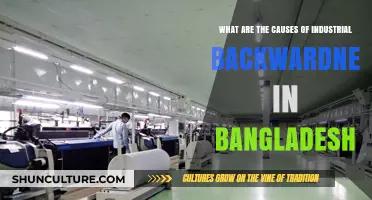
Prematurity and low birth weight: Leading cause due to inadequate prenatal care and maternal malnutrition
In Bangladesh, prematurity and low birth weight are the silent culprits behind a staggering number of neonatal deaths, accounting for nearly 30% of all cases. These conditions, often intertwined, stem from a lack of adequate prenatal care and pervasive maternal malnutrition. The consequences are dire: underdeveloped organs, weakened immune systems, and heightened susceptibility to infections like sepsis and pneumonia. For a nation striving to reduce its neonatal mortality rate, addressing these root causes is not just a health imperative but a moral obligation.
Consider the stark reality: a mother in rural Bangladesh, malnourished herself, gives birth to a baby weighing just 1.5 kilograms. Without access to proper prenatal care, her child faces an uphill battle for survival. Low birth weight infants are 40 times more likely to die in their first month compared to those born at a healthy weight. The solution lies in early intervention—ensuring mothers receive essential nutrients like iron, folic acid, and calcium during pregnancy. For instance, daily supplementation of 30-60 mg of iron and 400 mcg of folic acid can significantly reduce the risk of preterm birth and low birth weight. Pairing this with regular antenatal check-ups, where healthcare providers monitor fetal growth and maternal health, could be transformative.
However, the challenge extends beyond supplementation. Maternal malnutrition in Bangladesh is often a symptom of deeper socio-economic issues—poverty, food insecurity, and limited access to healthcare. A persuasive argument can be made for integrating nutrition education into community health programs. Teaching women about the importance of a balanced diet, rich in proteins, vitamins, and minerals, empowers them to make informed choices. For example, incorporating locally available foods like lentils, leafy greens, and fortified rice can combat nutrient deficiencies without straining limited resources.
Comparatively, countries like Sri Lanka have demonstrated success in reducing neonatal mortality by prioritizing maternal health. Bangladesh can draw lessons from such models by investing in grassroots initiatives that combine healthcare access with nutritional support. Mobile clinics, for instance, could bring prenatal services to remote areas, while community kitchens could provide nutritious meals to pregnant women. These steps, though resource-intensive, offer a sustainable path to breaking the cycle of prematurity and low birth weight.
In conclusion, tackling prematurity and low birth weight in Bangladesh requires a multi-faceted approach. From individual interventions like nutrient supplementation to systemic changes in healthcare delivery, every effort counts. By addressing maternal malnutrition and improving prenatal care, Bangladesh can not only save neonatal lives but also pave the way for healthier generations to come. The time to act is now—because every child deserves a fighting chance at survival.
Exploring Bangladesh's Diverse Regions: Geography, Culture, and Traditions
You may want to see also
Explore related products






![]()
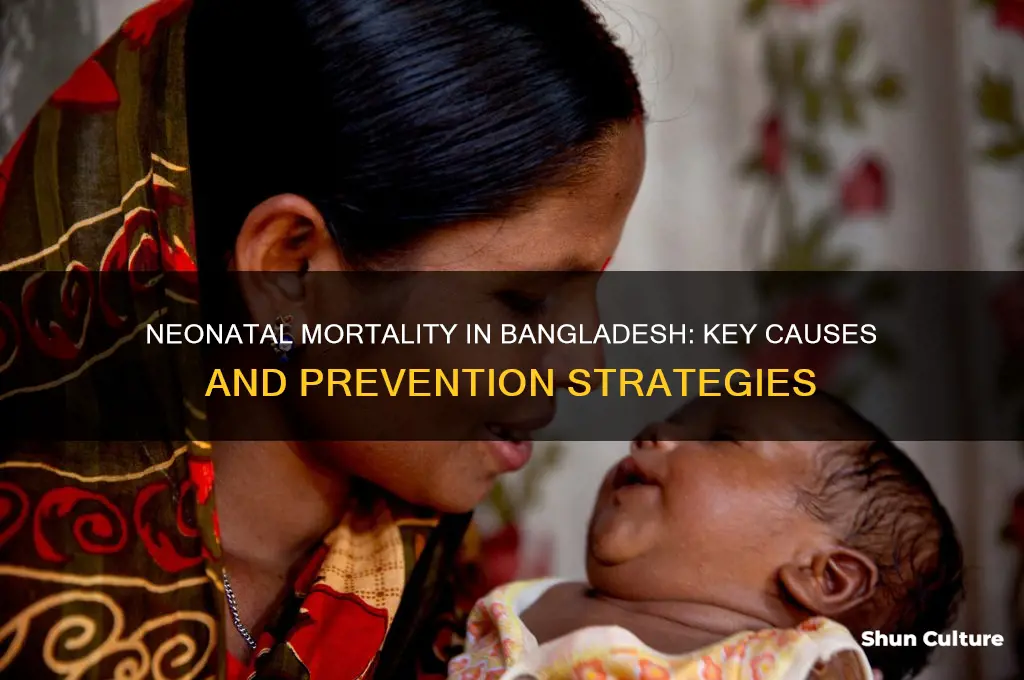
Neonatal infections: Sepsis, pneumonia, and meningitis contribute significantly to mortality rates
Neonatal infections, particularly sepsis, pneumonia, and meningitis, are among the leading causes of mortality in Bangladesh, accounting for a significant proportion of deaths within the first 28 days of life. These infections often arise from a combination of factors, including premature birth, low birth weight, and exposure to unsanitary conditions during delivery. For instance, in rural areas where access to healthcare facilities is limited, home births without sterile equipment or trained attendants increase the risk of bacterial contamination. The World Health Organization (WHO) highlights that early-onset sepsis, occurring within the first 72 hours of life, is frequently linked to maternal infections, while late-onset sepsis, after 72 hours, is often hospital-acquired or community-associated.
Sepsis, a life-threatening condition caused by the body’s extreme response to infection, is particularly devastating in neonates due to their underdeveloped immune systems. Symptoms such as lethargy, poor feeding, and respiratory distress are often nonspecific, delaying diagnosis. Treatment typically involves broad-spectrum antibiotics like ampicillin (50 mg/kg every 12 hours) and gentamicin (4-5 mg/kg every 48 hours), administered intravenously. However, the lack of diagnostic tools in resource-limited settings often results in empirical treatment, which may not always target the causative pathogen effectively. Early recognition and prompt antibiotic therapy are critical, as delays can lead to septic shock and multiorgan failure.
Pneumonia, another major contributor to neonatal mortality, is often caused by pathogens such as *Streptococcus pneumoniae* and *Haemophilus influenzae*. Preterm infants are especially vulnerable due to their immature lungs and weakened immune defenses. Clinical signs include tachypnea (respiratory rate >60 breaths/minute), grunting, and hypoxia. Management includes oxygen therapy, antibiotics like amoxicillin (75-90 mg/kg/day), and supportive care. Prevention strategies, such as exclusive breastfeeding and reducing indoor air pollution from cooking fuels, can significantly lower the incidence of pneumonia in neonates.
Meningitis, though less common than sepsis or pneumonia, carries a high mortality rate and long-term neurological sequelae. Neonatal meningitis is primarily caused by *Escherichia coli*, *Streptococcus agalactiae* (Group B Streptococcus), and *Listeria monocytogenes*. Symptoms include irritability, bulging fontanelle, and seizures. Treatment requires hospitalization for intravenous antibiotics such as cefotaxime (50 mg/kg every 6 hours) and ampicillin, often in combination with an aminoglycoside. Lumbar puncture, though essential for diagnosis, is frequently deferred in low-resource settings due to perceived risks, leading to reliance on clinical judgment and empirical treatment.
Addressing neonatal infections in Bangladesh requires a multifaceted approach. Strengthening healthcare infrastructure, particularly in rural areas, is essential to ensure access to sterile delivery practices and early postnatal care. Training healthcare workers to recognize early signs of infection and administer appropriate antibiotics can significantly reduce mortality. Additionally, community education on hygiene practices, antenatal care, and the importance of seeking medical attention for sick neonates is crucial. By targeting sepsis, pneumonia, and meningitis through prevention, early diagnosis, and effective treatment, Bangladesh can make substantial strides in reducing its neonatal mortality rate.
Travel Guide: Bangladesh to Poland - Visa, Flights, and Tips
You may want to see also
Explore related products






![]()
Birth asphyxia: Oxygen deprivation during delivery remains a critical factor in neonatal deaths
Birth asphyxia, a condition where newborns suffer from oxygen deprivation during delivery, is a leading cause of neonatal mortality in Bangladesh. Despite advancements in maternal and child healthcare, this critical issue persists, particularly in rural and underserved areas. The lack of immediate access to skilled birth attendants and essential medical equipment exacerbates the risk, leaving newborns vulnerable during the crucial moments of childbirth. Understanding the factors contributing to birth asphyxia is the first step toward mitigating its devastating impact.
One of the primary causes of birth asphyxia in Bangladesh is prolonged or obstructed labor, often due to inadequate prenatal care and delayed access to emergency obstetric services. For instance, in remote regions, women may travel hours to reach a healthcare facility, increasing the likelihood of complications during delivery. Additionally, cultural practices and misconceptions about childbirth sometimes deter families from seeking timely medical intervention. Educating communities about the importance of prenatal check-ups and recognizing danger signs during labor can significantly reduce the incidence of asphyxia.
The role of healthcare infrastructure cannot be overstated in addressing this issue. Many facilities in Bangladesh lack the necessary equipment, such as fetal heart rate monitors and resuscitation devices, to manage asphyxia effectively. Training healthcare providers in neonatal resuscitation techniques is equally critical. The World Health Organization (WHO) recommends the "Helping Babies Breathe" program, which has been implemented in several low-resource settings with promising results. By equipping facilities with basic tools and training staff, Bangladesh can improve its capacity to respond to asphyxia cases promptly.
Prevention strategies must also focus on high-risk pregnancies, which are more likely to result in birth asphyxia. Conditions like maternal hypertension, diabetes, and infections increase the risk of complications during delivery. Regular antenatal care, including screenings for these conditions, can help identify and manage risks early. For example, administering magnesium sulfate to pregnant women with severe preeclampsia has been shown to reduce the risk of neonatal mortality by preventing seizures and improving fetal outcomes.
Finally, raising awareness among families and communities is essential for long-term success. Simple interventions, such as ensuring a clean birthing environment and promoting immediate skin-to-skin contact between mother and baby, can improve neonatal survival rates. Community health workers play a vital role in disseminating this information and encouraging positive behaviors. By combining individual, community, and systemic efforts, Bangladesh can make significant strides in reducing neonatal deaths due to birth asphyxia, ensuring a healthier start for its youngest citizens.
Step-by-Step Guide: Applying for a Thai Visa from Bangladesh
You may want to see also
Explore related products






![]()
Lack of skilled birth attendants: Limited access to trained healthcare providers increases risks during childbirth
In Bangladesh, the absence of skilled birth attendants during childbirth significantly elevates the risk of neonatal mortality. Data from the Bangladesh Demographic and Health Survey reveals that only 42% of births are attended by trained healthcare providers, leaving a vast majority of mothers and newborns vulnerable. This gap in skilled care is particularly pronounced in rural areas, where traditional birth attendants, often lacking formal training, are the primary caregivers. Without the expertise to manage complications like obstructed labor, postpartum hemorrhage, or neonatal asphyxia, these situations frequently turn fatal. The stark disparity in access to skilled attendants between urban and rural regions underscores a critical public health challenge.
Consider the scenario of a mother in a remote village experiencing a prolonged labor. Without a skilled attendant, there is no one to recognize the signs of fetal distress or administer life-saving interventions like vacuum extraction or emergency referrals. In contrast, a mother in an urban hospital with access to a trained midwife or doctor is far more likely to receive timely care, such as neonatal resuscitation or antibiotics for infection. This comparison highlights how the presence or absence of skilled attendants directly correlates with neonatal survival rates. Practical steps to bridge this gap include deploying community health workers trained in basic emergency obstetric care and establishing referral systems to link rural areas with urban healthcare facilities.
Persuasively, investing in skilled birth attendants is not just a moral imperative but a cost-effective strategy to reduce neonatal deaths. Studies show that increasing the proportion of births attended by skilled providers could avert up to 25% of neonatal fatalities in Bangladesh. Governments and NGOs must prioritize training programs for midwives and nurses, focusing on rural areas where the need is most acute. Additionally, incentivizing healthcare providers to work in underserved regions through salary supplements or career advancement opportunities could help address the urban-rural divide. Without such interventions, the cycle of preventable neonatal deaths will persist, hindering progress toward global health goals.
Descriptively, the impact of skilled birth attendants extends beyond immediate childbirth. These providers also offer essential postnatal care, such as counseling on breastfeeding, cord care, and recognizing danger signs in newborns. For instance, a trained midwife can educate a mother on the importance of initiating breastfeeding within the first hour of birth, a practice proven to reduce neonatal mortality by 22%. Similarly, they can identify and treat infections early, preventing complications that often lead to death in resource-limited settings. By integrating skilled attendants into the continuum of care, Bangladesh can create a safety net that protects both mothers and newborns from avoidable risks.
In conclusion, the lack of skilled birth attendants in Bangladesh is a critical driver of neonatal mortality, particularly in rural areas. Addressing this issue requires a multi-faceted approach, including training more healthcare providers, improving access to emergency obstetric care, and raising awareness about the importance of skilled attendance at birth. By prioritizing these measures, Bangladesh can significantly reduce neonatal deaths and move closer to achieving its health development targets. The lives of countless newborns depend on it.
Exploring Bangladesh: Unveiling the Total Number of Villages Nationwide
You may want to see also
Explore related products






![]()
Poor healthcare infrastructure: Inadequate facilities and resources hinder timely and effective neonatal care
In Bangladesh, the stark reality is that many neonatal deaths could be prevented with timely and effective healthcare interventions. However, the country’s poor healthcare infrastructure often stands as an insurmountable barrier. Rural areas, where the majority of the population resides, are particularly affected. Clinics and hospitals in these regions frequently lack basic equipment such as incubators, phototherapy units, and even reliable electricity. For instance, a study found that only 30% of healthcare facilities in rural Bangladesh have functional neonatal intensive care units (NICUs), leaving newborns with critical conditions like sepsis or respiratory distress syndrome without adequate treatment options.
Consider the logistical challenges faced by families in remote villages. When a newborn requires urgent care, the nearest equipped facility might be hours away, often inaccessible due to poor road conditions or lack of transportation. Even if they reach a hospital, overcrowding and understaffing mean long wait times, during which a newborn’s condition can deteriorate rapidly. For example, a baby with severe jaundice needs immediate phototherapy, but if the hospital’s only machine is in use, the delay can lead to irreversible brain damage or death. This highlights how inadequate infrastructure directly translates to missed opportunities for survival.
The resource gap extends beyond equipment to essential supplies and trained personnel. Many facilities lack access to lifesaving medications like antibiotics, surfactants, or even basic intravenous fluids. Additionally, there is a severe shortage of trained healthcare providers, particularly neonatal specialists. In Bangladesh, there is approximately one pediatrician for every 20,000 children, and even fewer with specialized training in neonatal care. This shortage forces general practitioners or nurses to manage complex cases, often without adequate support or guidelines, increasing the risk of misdiagnosis or inappropriate treatment.
To address this crisis, targeted investments in healthcare infrastructure are critical. This includes not only building new facilities but also upgrading existing ones with essential equipment and ensuring a steady supply of medications and consumables. Mobile health units equipped with basic neonatal care tools could bridge the gap in remote areas, providing immediate interventions while arranging transfers to better-equipped hospitals. Simultaneously, scaling up training programs for healthcare workers in neonatal care, particularly in rural areas, can empower local staff to handle emergencies more effectively.
Ultimately, the link between poor healthcare infrastructure and neonatal mortality in Bangladesh is undeniable. While broader systemic changes are needed, immediate steps such as equipping facilities, improving access, and training personnel can make a tangible difference. Every functional incubator, every trained nurse, and every accessible clinic brings Bangladesh one step closer to reducing its neonatal mortality rate and ensuring that more newborns survive their first critical days of life.
Understanding Bangladesh Overruns: Causes, Impacts, and Solutions Explained
You may want to see also
Frequently asked questions
The primary causes of neonatal death in Bangladesh include preterm birth complications, neonatal infections (such as sepsis and pneumonia), birth asphyxia, and congenital anomalies.
Preterm birth is a major contributor to neonatal deaths in Bangladesh, accounting for a substantial proportion of fatalities due to underdeveloped organs and increased susceptibility to infections.
Neonatal infections, particularly sepsis and pneumonia, are critical causes of mortality, often resulting from poor hygiene during delivery, lack of access to clean healthcare facilities, and inadequate postnatal care.
Congenital anomalies, such as heart defects and neural tube defects, significantly contribute to neonatal deaths in Bangladesh, often due to limited access to advanced diagnostic and treatment facilities.