Iron deficiency anemia is a prevalent public health concern in Bangladesh, affecting a significant portion of its population, particularly women and children. The high incidence can be attributed to several factors, including poor dietary intake of iron-rich foods, limited access to diverse and nutritious meals, and inadequate absorption of iron due to concurrent infections such as parasitic infestations. Additionally, cultural practices, socioeconomic disparities, and a reliance on staple foods like rice, which are low in iron, exacerbate the problem. Women of reproductive age and pregnant women are especially vulnerable due to increased iron demands, while children face higher risks due to rapid growth and development. Addressing this issue requires multifaceted interventions, including nutritional education, food fortification, and improved healthcare access to combat underlying causes and reduce the burden of anemia in the country.
| Characteristics | Values |
|---|---|
| Prevalence of Iron Deficiency Anemia (IDA) | Approximately 42% of children under 5 and 27% of non-pregnant women in Bangladesh suffer from IDA (Source: Bangladesh Demographic and Health Survey, 2022). |
| Dietary Factors | Low consumption of iron-rich foods (e.g., red meat, poultry, fish) due to poverty and limited access to diverse diets. High reliance on rice, which has low iron content and inhibits iron absorption. |
| Hookworm Infections | High prevalence of hookworm infections (affecting ~15% of the population) leads to chronic blood loss and reduced iron absorption (Source: WHO, 2021). |
| Menstrual Blood Loss | Women of reproductive age are at higher risk due to menstrual blood loss, with limited access to iron supplements or fortified foods. |
| Pregnancy and Lactation | Increased iron demand during pregnancy and lactation, coupled with inadequate dietary intake, exacerbates IDA prevalence (affecting ~42% of pregnant women). |
| Malaria and Intestinal Parasites | Endemic malaria and intestinal parasites (e.g., Giardia, Entamoeba) contribute to chronic inflammation and impaired iron absorption. |
| Limited Access to Fortified Foods | Low availability and consumption of iron-fortified foods (e.g., flour, oil) due to economic constraints and lack of awareness. |
| Poor Sanitation and Hygiene | Inadequate sanitation and hygiene practices increase the risk of infections that exacerbate IDA. |
| Genetic Factors | Prevalence of genetic hemoglobin disorders (e.g., thalassemia) in certain regions, which can coexist with or mimic IDA. |
| Healthcare Access | Limited access to healthcare services, including prenatal care and iron supplementation programs, particularly in rural areas. |
| Awareness and Education | Low awareness about IDA prevention, symptoms, and treatment options among the general population. |
Explore related products





What You'll Learn
- Poor Dietary Intake: Limited access to iron-rich foods like meat, fish, and leafy greens
- Chronic Blood Loss: Hookworm infections and heavy menstrual bleeding contribute to anemia
- High Disease Burden: Malaria and gastrointestinal disorders impair iron absorption and cause loss
- Poverty and Malnutrition: Economic constraints limit access to nutritious food and healthcare
- Lack of Awareness: Insufficient education on iron deficiency prevention and treatment measures
![]()
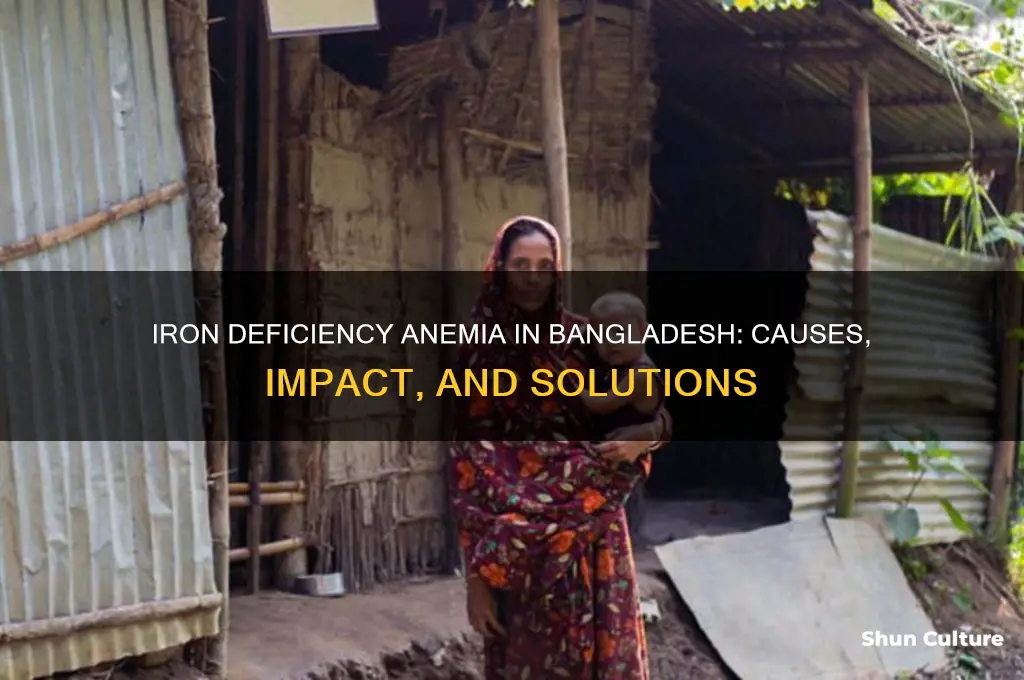
Poor Dietary Intake: Limited access to iron-rich foods like meat, fish, and leafy greens
In Bangladesh, a staggering 42% of women of reproductive age suffer from iron deficiency anemia, a condition exacerbated by poor dietary intake. The root cause? Limited access to iron-rich foods like meat, fish, and leafy greens. These foods are not only expensive but also scarce in many regions, particularly rural areas where 60% of the population resides. For instance, a kilogram of beef costs approximately 600 BDT (7 USD), a luxury for families living on less than 2 USD a day. Without these essential sources of heme iron—the most absorbable form—the body struggles to maintain adequate iron levels, leading to anemia.
Consider the daily diet of a typical rural Bangladeshi family. Staples like rice and lentils dominate meals, providing calories but little iron. Leafy greens, though rich in non-heme iron, are often unavailable due to seasonal shortages or lack of cultivation. Fish, a more affordable protein source, is consumed irregularly, especially in landlocked areas. To combat this, households should aim to include at least one iron-rich food daily. For example, adding a handful of spinach (2.7 mg iron per 100g) to a lentil curry or incorporating small fish like shad (3.2 mg iron per 100g) into meals can make a significant difference. Pairing these with vitamin C-rich foods like lemons or amla (Indian gooseberry) enhances iron absorption by up to 300%.
However, access alone isn’t the issue—awareness is equally critical. Many Bangladeshis are unaware of the importance of dietary diversity or how to maximize iron absorption. For instance, drinking tea with meals, a common practice, inhibits iron absorption due to its tannins. Simple changes, like consuming tea between meals instead of during, can improve iron uptake. Additionally, fortified foods like iron-rich flour or oil could be game-changers, but their availability remains limited. Government and NGO initiatives should focus on educating communities about affordable, locally available iron sources and promoting kitchen gardens to grow spinach, fenugreek, or mustard greens.
Comparatively, countries like Thailand and Vietnam have successfully tackled anemia through agricultural diversification and public health campaigns. Bangladesh can draw lessons by integrating iron-rich crops into existing farming systems and subsidizing livestock rearing for poorer households. For pregnant women and children under five—the most vulnerable groups—targeted interventions like iron supplements (60 mg/day for adults, 10 mg/day for children) should be paired with dietary counseling. Without addressing these gaps, the cycle of anemia will persist, hindering cognitive development, productivity, and overall health.
Understanding the Structure and Format of a Bangladesh Phone Number
You may want to see also
Explore related products






![]()
Chronic Blood Loss: Hookworm infections and heavy menstrual bleeding contribute to anemia
In Bangladesh, chronic blood loss is a silent yet pervasive contributor to the high prevalence of iron deficiency anemia, particularly in rural areas. One major culprit is hookworm infection, a parasitic disease that thrives in environments with poor sanitation and open defecation practices. Hookworms attach to the intestinal wall, feeding on blood and causing ongoing, often unnoticed, blood loss. Over time, this can deplete iron stores, leading to anemia. Studies show that hookworm infections are endemic in regions with limited access to clean water and proper sanitation, affecting up to 50% of the population in some rural communities. For individuals infected, the daily blood loss can range from 0.1 to 0.3 ml per worm, with heavy infections involving hundreds of parasites, exacerbating iron deficiency.
Another significant yet underaddressed cause of chronic blood loss is heavy menstrual bleeding (menorrhagia), which disproportionately affects women of reproductive age in Bangladesh. Cultural taboos surrounding menstruation often prevent open discussions, delaying diagnosis and treatment. Women with menorrhagia can lose over 80 ml of blood per menstrual cycle, compared to the average 30–40 ml, significantly increasing their risk of anemia. Factors such as inadequate access to menstrual hygiene products, malnutrition, and lack of awareness about gynecological health further compound the issue. For instance, a survey in rural Bangladesh found that only 12% of women sought medical advice for heavy bleeding, often attributing it to "normal" menstrual discomfort.
Addressing these causes requires a multi-pronged approach. For hookworm infections, mass drug administration (MDA) programs using albendazole or mebendazole (400 mg single dose) have proven effective in reducing prevalence. However, MDA must be paired with improvements in sanitation, such as building latrines and promoting the use of footwear to prevent reinfection. Schools and community centers can serve as hubs for education on hygiene practices, targeting children and adults alike. For heavy menstrual bleeding, healthcare providers should screen women during routine check-ups, using tools like the Pictorial Blood Loss Assessment Chart to quantify blood loss. Treatment options include iron supplementation (60–100 mg elemental iron daily), tranexamic acid to reduce bleeding, and hormonal therapies like the levonorgestrel intrauterine system (LNG-IUS) for long-term management.
Practical tips for individuals include maintaining a diet rich in iron (e.g., leafy greens, lentils, and fortified foods) and pairing iron sources with vitamin C to enhance absorption. Women experiencing heavy periods should track their symptoms using mobile apps or journals to provide accurate information to healthcare providers. Community health workers can play a vital role in destigmatizing menstruation and educating women about available resources. By tackling both hookworm infections and menorrhagia head-on, Bangladesh can make significant strides in reducing the burden of iron deficiency anemia and improving overall public health.
Exploring Bangladesh's Unique Name for Salmon Fish: A Culinary Insight
You may want to see also
Explore related products




![]()
High Disease Burden: Malaria and gastrointestinal disorders impair iron absorption and cause loss
Malaria and gastrointestinal disorders are silent saboteurs of iron levels in Bangladesh, exacerbating the country’s anemia crisis. Malaria, endemic in many regions, triggers hemolysis—the destruction of red blood cells—leading to acute iron loss. Simultaneously, chronic gastrointestinal infections, rampant due to contaminated water and poor sanitation, impair nutrient absorption in the small intestine, where iron is primarily absorbed. This dual assault creates a vicious cycle: disease depletes iron, and iron deficiency weakens immunity, making individuals more susceptible to these very diseases.
Consider the mechanism: Giardia, a common parasite in Bangladesh’s water sources, damages intestinal villi, reducing surface area for nutrient uptake. Studies show that even mild giardiasis can decrease iron absorption by up to 50%. For children under five, who require 7–10 mg of iron daily for growth, this disruption is catastrophic. Adults fare no better; chronic diarrhea from conditions like amoebiasis or bacterial infections further depletes iron stores through fecal loss. Without addressing these infections, iron supplementation alone becomes a futile effort.
Malaria compounds the problem. Each episode of Plasmodium falciparum malaria, prevalent in Bangladesh’s rural areas, destroys millions of red blood cells, releasing heme that the body struggles to recycle. This not only causes immediate iron loss but also triggers inflammation, which inhibits iron release from storage sites like the liver. For pregnant women, who need 27 mg of iron daily, malaria-induced anemia increases the risk of maternal mortality and low-birth-weight infants. The World Health Organization estimates that 30% of anemia cases in malaria-endemic regions are directly linked to the disease.
Breaking this cycle requires a two-pronged approach. First, disease prevention: distributing insecticide-treated bed nets reduces malaria transmission, while water purification tablets and sanitation programs curb gastrointestinal infections. Second, targeted nutrition: pair iron supplements with vitamin A (which enhances iron absorption) and administer them during disease-free periods. For example, seasonal malaria chemoprevention campaigns can include iron distribution for at-risk groups. Without addressing these underlying diseases, iron deficiency anemia in Bangladesh will persist, undermining public health and economic productivity.
Exploring the Diverse Varieties of Mangoes in Bangladesh
You may want to see also
Explore related products





![]()
Poverty and Malnutrition: Economic constraints limit access to nutritious food and healthcare
In Bangladesh, where nearly 25% of the population lives below the poverty line, economic constraints create a vicious cycle that perpetuates iron deficiency anemia. Poverty limits access to diverse, nutrient-rich foods, forcing families to rely on inexpensive, calorie-dense but nutrient-poor staples like polished rice. A 2011 study by the Bangladesh Bureau of Statistics revealed that 60% of households in rural areas cannot afford a diet that meets the recommended daily iron intake of 18 mg for adults and 27 mg for pregnant women. This dietary inadequacy is compounded by the high cost of iron-fortified foods and supplements, which are often beyond the reach of low-income families.
Consider the daily struggle of a mother in a rural village, earning less than $2 a day, trying to feed her family. She might spend 70% of her income on food, yet still fall short of providing the necessary iron-rich foods like red meat, poultry, or leafy greens. Instead, her family consumes rice-based meals, which provide energy but lack essential micronutrients. This dietary pattern, coupled with limited access to healthcare, increases the risk of iron deficiency anemia, particularly among women and children. For instance, the World Health Organization reports that 42% of children under five in Bangladesh are anemic, a statistic directly linked to poor dietary diversity and economic hardship.
To break this cycle, targeted interventions are essential. One practical step is promoting low-cost, iron-rich foods such as lentils, spinach, and fortified soy products, which can provide up to 6 mg of iron per serving. Community-based nutrition programs can educate families on preparing these foods effectively, such as pairing iron sources with vitamin C-rich foods like lemons or tomatoes to enhance absorption. Additionally, governments and NGOs can implement food fortification programs, as seen in Bangladesh’s success with iodized salt, to address widespread deficiencies. For example, fortifying widely consumed staples like rice or oil with iron could significantly improve intake without increasing household expenses.
However, addressing malnutrition requires more than dietary adjustments. Economic empowerment is crucial. Microfinance initiatives and vocational training can provide families with the means to afford better nutrition and healthcare. For instance, a study by BRAC, a Bangladeshi NGO, found that women participating in microfinance programs were 20% more likely to seek prenatal care, which includes iron supplementation. Similarly, school feeding programs that incorporate iron-rich foods can improve children’s health while reducing the financial burden on families. These multifaceted approaches not only combat anemia but also address the root cause of poverty, creating a sustainable solution for future generations.
Ultimately, the link between poverty and iron deficiency anemia in Bangladesh underscores the need for integrated strategies that combine nutrition, healthcare, and economic development. Without addressing the economic constraints that limit access to nutritious food and medical care, efforts to reduce anemia will remain incomplete. By focusing on affordable, sustainable solutions and empowering communities, Bangladesh can make significant strides in improving public health and breaking the cycle of poverty-induced malnutrition.
Bangladesh's Upcoming ODI Series Schedule: Dates and Opponents Revealed
You may want to see also
Explore related products






![]()
Lack of Awareness: Insufficient education on iron deficiency prevention and treatment measures
In Bangladesh, a staggering 42% of non-pregnant women and 32% of children under five suffer from iron deficiency anemia, according to the National Micronutrient Survey 2013. These numbers aren't just statistics; they represent millions of individuals grappling with fatigue, weakened immunity, and impaired cognitive function due to a lack of this essential mineral. While factors like dietary inadequacy and parasitic infections contribute, a critical piece of the puzzle lies in the shadows: a pervasive lack of awareness about iron deficiency prevention and treatment.
Imagine a mother, unaware that her child's pale complexion and lethargy could be signs of anemia, attributing it to "growing pains" instead. This scenario isn't uncommon in Bangladesh, where limited access to health education leaves many vulnerable to this preventable condition.
The consequences of this knowledge gap are far-reaching. Pregnant women, for instance, require nearly double the daily iron intake (27 mg) compared to non-pregnant women (18 mg) to support both their own needs and their developing fetus. Without this knowledge, they risk maternal anemia, low birth weight, and even increased mortality rates for both mother and child. Similarly, children, especially those under two, are at high risk due to their rapid growth and often limited diets. Introducing iron-rich foods like lentils, spinach, and fortified cereals alongside vitamin C-rich foods to enhance absorption is crucial, yet this information often remains inaccessible to many families.
This lack of awareness isn't merely a knowledge deficit; it's a systemic issue. Rural areas, where healthcare infrastructure is often inadequate, are particularly affected. Traditional beliefs and cultural practices sometimes contradict evidence-based recommendations, further complicating matters. For example, the misconception that excessive tea consumption can replace iron-rich foods persists, hindering effective prevention strategies.
Bridging this awareness gap requires a multi-pronged approach. Community health workers, trained to deliver culturally sensitive information, can play a pivotal role in educating families about iron-rich foods, supplementation when necessary, and recognizing anemia symptoms. Mass media campaigns, utilizing local languages and culturally relevant messaging, can reach a wider audience. Schools can incorporate nutrition education into their curricula, empowering children to make informed choices and become advocates for healthier lifestyles within their families. By addressing this lack of awareness, Bangladesh can take a significant step towards combating the pervasive problem of iron deficiency anemia and ensuring a healthier future for its population.
Easy Steps to Call Dhaka, Bangladesh from the USA
You may want to see also
Frequently asked questions
Iron deficiency anemia is common in Bangladesh due to poor dietary intake of iron-rich foods, limited access to diverse nutrition, and high prevalence of parasitic infections like hookworm, which deplete iron levels.
The typical Bangladeshi diet often lacks sufficient iron-rich foods such as red meat, leafy greens, and fortified products. Instead, it relies heavily on polished rice, which has low iron content, exacerbating the deficiency.
Parasitic infections, particularly hookworm, are widespread in Bangladesh due to poor sanitation and hygiene. These parasites cause chronic blood loss in the intestines, leading to reduced iron levels and anemia.
Yes, women and children are disproportionately affected due to increased iron demands during pregnancy, menstruation, and growth. Limited access to healthcare and nutrition further exacerbates the problem in these vulnerable groups.