Australia's healthcare system is a shared public-private model underpinned by Medicare, the national single-payer funding model. Medicare has been Australia's universal healthcare scheme since 1984 and is available to citizens, permanent residents, and some visitors and visa holders. It covers the cost of public hospital services and some or all of the costs of other health services, including GPs, medical specialists, physiotherapy, community nurses, and basic dental services for children. The Pharmaceutical Benefits Scheme (PBS), which predates Medicare, subsidises certain prescribed pharmaceuticals, making them more affordable. The COVID-19 pandemic impacted health spending, and in 2022, Australia's health spending to GDP ratio was 9.9%, ranking 15th among 38 OECD member countries. While Medicare provides free or low-cost access to healthcare, private health insurance is also available, with two types of cover: hospital cover and general treatment cover for non-medical services not covered by Medicare. Out-of-pocket fees are a concern, with 15% of healthcare expenditure coming directly from individuals, and vulnerable groups spending larger proportions of their incomes on healthcare.
| Characteristics | Values |
|---|---|
| Health spending to GDP ratio in 2022 | 9.9% |
| Ranking of health spending to GDP ratio in 2022 among 38 OECD countries | 15th |
| Health spending to GDP ratio from 2014 to 2018 | 9.8% to 10.1% |
| Health spending to GDP ratio in 2020 | 10.7% |
| Health spending to GDP ratio in 2021 | 10.4% |
| Percentage of health care expenditure from individuals | 15% |
| Average salary of specialists before tax | $400,000 per year |
| Average salary of GPs before tax | $200,000 per year |
| Number of physicians per 1000 population in 2015 | 3.52 |
| Number of hospital beds per 1000 population in 2022-23 | 2.5 |
| Number of medical practitioners in 2011 | 70,200 |
| Number of nurses in 2011 | 257,200 |
| Rate of medical practitioners per 100,000 population in 2012 | 374 |
| Rate of nurses and midwives per 100,000 population in 2012 | 1,124 |
Explore related products






What You'll Learn
![]()
Medicare and public hospital systems
Australia's health care system operates on a shared public-private model, with Medicare serving as the national single-payer funding model. Medicare has been Australia's universal healthcare scheme since 1984 and is available to citizens, permanent residents, and some visitors and visa holders. It covers the cost of public hospital services and some or all of the costs of other health services, including GPs, medical specialists, physiotherapy, community nurses, and basic dental services for children.
The Pharmaceutical Benefits Scheme (PBS), which predates Medicare, having been established in 1948, is considered a separate health policy. The PBS subsidises certain prescribed pharmaceuticals, making medicines cheaper and more accessible. Without the PBS, some medicines would cost tens of thousands of dollars more. Medicare and the PBS have safety nets that help cover the cost of healthcare and medicines for those with high out-of-pocket expenses.
The public hospital system, in conjunction with Medicare, provides free or low-cost access to healthcare services for all Australians. State and territory governments operate these public health facilities, and eligible patients receive care at no charge. Primary health services, such as GP clinics, are mostly privately owned but attract Medicare rebates.
While Medicare and the public hospital system provide universal coverage, many Australians opt for private health insurance to access private healthcare services outside the public system. Private health insurance covers hospital treatment as a private patient and general treatment for non-medical services not covered by Medicare, such as dental, physiotherapy, and optical services. The Australian government provides a rebate to assist with private health insurance costs.
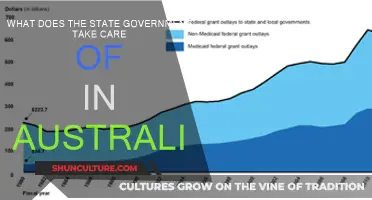
The cost of healthcare in Australia has been impacted by various factors, including the COVID-19 pandemic, advances in medical science, and new technologies. In 2022, Australia's health spending to GDP ratio was 9.9%, ranking 15th among 38 OECD member countries.
Australian Dollars: Understanding the Value of 99
You may want to see also
Explore related products

$23.24 $24.99

$57.99 $105.95




![]()
Private health insurance
There are two types of private health insurance cover: hospital cover and general treatment cover. Hospital cover includes some or all of the costs of hospital treatment as a private patient, whereas general treatment cover, also known as 'ancillary' or 'extras' cover, includes non-medical health services. Some people with private health insurance have either hospital cover or extras cover, while others have both.
Private healthcare services in Australia are provided through the market, allowing providers to set their own fees to cover operational costs and make profits. This has raised concerns about equity, as out-of-pocket fees do not directly subsidize access for people of lower socioeconomic status. Furthermore, public subsidization of private health insurance premiums has led to criticism that public expenditure may be transferred to wealthier individuals rather than those more in need of care.
GST in Australia: When Does It Apply?
You may want to see also
Explore related products






![]()
Out-of-pocket fees
In Australia, 15% of all expenditure on healthcare comes directly from individuals in the form of out-of-pocket fees, almost double the amount contributed by private health insurers. Out-of-pocket costs are also called gap or patient payments and refer to the difference between the amount a doctor charges for a medical service and what Medicare and any private health insurer pays.
The Australian healthcare system is a mix of public and private providers, with governments subsidising the costs of care. Medicare, Australia's universal healthcare scheme since 1984, covers the cost of public hospital services and some or all of the costs of other health services. These can include services provided by GPs and medical specialists, as well as physiotherapy, community nurses, and basic dental services for children. The Pharmaceutical Benefits Scheme (PBS), a part of Medicare, helps make medicines cheaper.
Private healthcare services, on the other hand, are provided through the market, where providers can set their own fees to cover operational costs and make profits. This results in higher fees for private specialists and GPs, with the average salary before tax and after practice costs being around $400,000 per year for specialists and $200,000 per year for GPs.
While private health insurance can cover some out-of-hospital services that Medicare does not, such as physiotherapy, it cannot cover out-of-hospital Medicare services. This means that individuals may still need to pay out-of-pocket costs for services outside of the hospital, even with private health insurance.
The level of out-of-pocket fees in Australia has sparked debates around the impact of high fees on patient access to care and the equity implications, particularly for socio-economically disadvantaged individuals and older Australians with higher healthcare needs. A 2019 study found that one in three low-income households spends more than 10% of their income on healthcare, leading to potential economic hardship and avoidance of care due to cost concerns.
Colgate Toothpaste: Gluten-Free in Australia?
You may want to see also
Explore related products






![]()
Government subsidies
Australia's health-care system operates on a shared public-private model, with Medicare serving as the national single-payer funding model. Medicare, Australia's universal health-care scheme since 1984, provides free or low-cost access to most health-care services for Australian citizens, permanent residents, and some visitors and visa holders. It covers the cost of public hospital services and some or all of the costs of other health services, including GP visits, medical specialists, physiotherapy, community nurses, and basic dental services for children.
The Pharmaceutical Benefits Scheme (PBS), a separate health policy that predates Medicare, subsidises certain prescribed pharmaceuticals to make them more affordable. The Australian government pays the rest of the cost for most PBS medicines if the patient is enrolled in Medicare.
State and territory governments also administer peripheral health programs, such as free dentistry for school students and community sexual health programs. They also provide free or subsidised dental services to specific population categories, such as Health Care Card and Pensioner Concession Card holders.
The National Disability Insurance Scheme (NDIS) is another government-funded initiative that provides necessary support for people with disabilities to enable their participation in the economy and community.
The Australian government also provides a means-tested rebate to help with the cost of private health insurance, which offers choice outside the public system. The rebate scheme was introduced in 1999, and under it, the government contributes up to 30% of the private health insurance premium of people covered by Medicare.
While the public system is largely funded by the government, private health-care services are provided through the market, with fees covering staff salaries, capital costs, operation costs, and profits for private providers.
However, concerns have been raised about the impact of out-of-pocket fees on vulnerable groups, with one study finding that one in three low-income households spends more than 10% of their income on health care. There is also criticism that government subsidies for private health insurance premiums ($6.2 billion per year) may transfer public expenditure away from lower socioeconomic groups towards wealthier individuals.
Exploring Your Australian Home's History
You may want to see also
Explore related products






![]()
Dental care
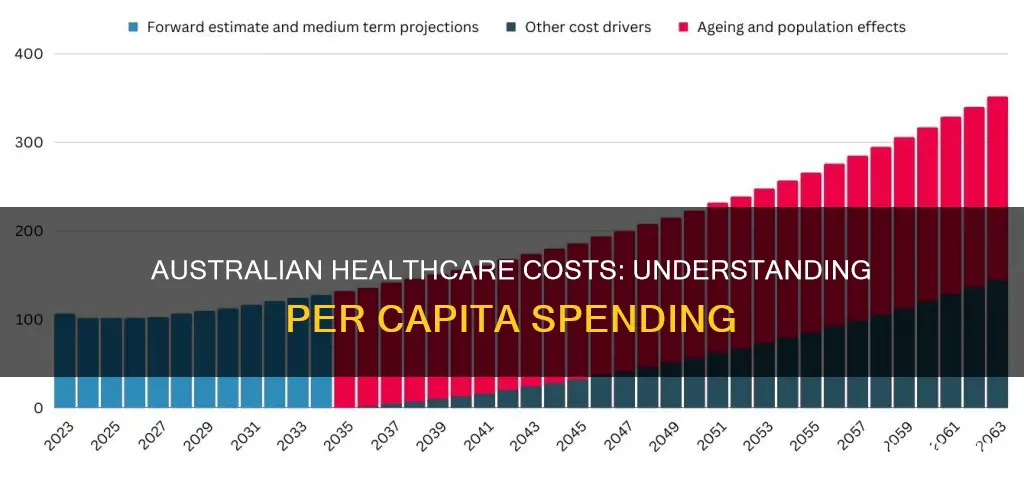
The Australian government spent $1.3 billion on dental services in 2021-22, with per capita expenditure on dental services at $432 in the same period. This is an increase from $390 in 2019-20 and a decrease from $438 in 2020-21. Overall, government expenditure on dental services has declined at an average annual rate of 3.6% over the last decade.
The high cost of dental care in Australia is a significant issue, with many people unable to afford treatment. This has resulted in a rise in untreated dental decay and oral health problems. In 2021-22, Australia ranked sixth out of 31 OECD countries for per capita expenditure on dental care, with around 60% of the $11.1 billion spent coming from individual out-of-pocket expenses.
To reduce the financial burden, many Australians use private health insurance to help pay for dental care. In 2017-18, around 50% of males and 54.3% of females aged 5 years and over had private health insurance cover for dental expenses. However, insurance policies vary widely, and the level of cover depends on the type of policy purchased. Some policies have limits on the total amount that can be claimed, and there may be waiting periods for additional coverage.
To reduce the cost of dental care, individuals can take preventive measures to maintain oral health. This includes practices such as regular brushing and flossing, as well as the use of fluoride in drinking water and toothpaste. Additionally, individuals can compare prices between dentists and ask about the necessity and alternatives for specific procedures.
A New Signature: Legally Changing Your Name in Australia
You may want to see also
Frequently asked questions
In 2022, Australia's health spending to GDP ratio ranked 15th out of 38 OECD member countries, with a ratio of 9.9% compared to the OECD median of 9.5%.
The Medicare levy is a 2% surcharge that funds Medicare, Australia's universal healthcare scheme. It applies to individuals over 35 who don't have private health insurance. Exemptions and reductions are available for low-income earners.
Medicare covers the full cost of public hospital services and some or all of the costs of other health services, including GPs, medical specialists, physiotherapy, community nurses, and basic dental services for children. However, it does not cover ambulance services, most dental care, glasses, contact lenses, hearing aids, or cosmetic surgery.
The PBS subsidises certain prescribed pharmaceuticals, making them more affordable for Australians. It is a separate policy from Medicare and is administered by the Department of Human Services Insurance.
Out-of-pocket fees and government subsidies have been criticised for potentially benefiting wealthier individuals while disadvantaging those from lower socioeconomic backgrounds who are more likely to need care. Vulnerable groups, such as socio-economically disadvantaged people and older Australians, may spend larger proportions of their incomes on healthcare, sometimes leading to economic hardship and foregone care.