Bolivia is the second poorest country in South America, with a poor performance in education, life expectancy, economic strength and overall development. It also lacks sufficient medical care due to a limited supply of resources. Cardiovascular diseases (CVDs) are the number one cause of death in Bolivia, and a study in Cochabamba, Bolivia, found that the prevalence of CVD risk factors in the region was high. However, there is a lack of reliable estimates of risk factor distribution, which can delay the implementation of evidence-based interventions.
The Tsimane people of the Bolivian Amazon have been found to have the healthiest hearts in the world, with heart attacks and strokes being almost unknown among them. This is attributed to their active lifestyle and diet, which consists of a high amount of carbohydrates, low amounts of fat and sugar, and about 15% protein. They also walk a lot, with men walking an average of 17,000 steps a day and women 16,000.
Explore related products


$8.48 $22




![]()
Diet
The Tsimane's diet is also a product of their lifestyle and environment. As subsistence farmers and foragers, they consume only what they can grow or catch, resulting in a very fresh and extremely low-fat diet. Their food is not processed or refined, and they do not add extra salt or sugar. This natural, whole-food diet is rich in micronutrients such as selenium, potassium, and magnesium, which are essential for maintaining heart health.
In addition to their healthy diet, the Tsimane also engage in regular physical activity. The men are physically active for 6 to 7 hours a day, while the women are active for 4 to 6 hours. On average, the Tsimane take about 17,000 steps a day, which is significantly more than the recommended amount for adults. This active lifestyle, combined with their healthy diet, helps to keep their hearts strong and reduces their risk of heart disease.
However, it is important to note that the Tsimane's diet and lifestyle are not easily replicable for those living in modern, urban environments. Their diet is born out of necessity and the availability of resources in their local environment. Additionally, their physical activity is not structured exercise but rather a result of their daily activities, such as hunting, farming, and foraging.
While we may not be able to replicate the Tsimane's exact diet and lifestyle, there are still lessons we can learn from them. Increasing our intake of whole foods, reducing our consumption of processed foods, and incorporating more physical activity into our daily routines can all contribute to improving our heart health. Additionally, the Tsimane's diet and lifestyle highlight the importance of cultural and environmental factors in shaping dietary patterns and health outcomes.
Bolivian Rams: Aggressive or Peaceful Fish for Your Aquarium?
You may want to see also
Explore related products

$12.99 $12.99





![]()
Lifestyle
Diet:
The diet of Bolivians can significantly impact their heart health. In Cochabamba, a cross-sectional community-based study found that 76.73% of participants had a low consumption of fruits and vegetables. This is a risk factor for cardiovascular disease (CVD), as a diet rich in fruits and vegetables is associated with a reduced risk. Additionally, the high consumption of carbohydrates and saturated fats in the typical Bolivian diet, along with the reuse of oils for frying and the increasing trend of fast food consumption, can contribute to heart disease. However, it's important to note that the Tsimane indigenous people, who follow a high-carbohydrate, low-protein diet, have been found to have the healthiest hearts globally due to their active lifestyle.
Physical Activity:
Lack of physical activity is another risk factor for CVD. In the Cochabamba study, 64.77% of participants reported low levels of physical activity. On the other hand, the Tsimane people's active lifestyle, which includes around six hours of daily exercise through hunting, farming, and foraging, contributes to their exceptional heart health.
Smoking and Alcohol Consumption:
Smoking and alcohol consumption are modifiable risk factors for CVD. In Cochabamba, 11.6% of participants were current smokers, and 42.76% reported current alcohol consumption. These behaviours can increase the likelihood of developing heart disease.
Obesity and Overweight:
Obesity and being overweight are prevalent in Bolivia and are risk factors for CVD. In the Cochabamba study, 35.84% of participants were overweight, and 20.49% were obese. These conditions can strain the heart and increase the risk of heart-related issues.
Socio-Economic Factors:
Socio-economic factors also play a role in lifestyle choices and heart disease risk. For example, people in rural areas may have limited access to healthcare services, healthy food options, and opportunities for physical activity. Additionally, education level can influence lifestyle choices, as those with lower education are more likely to engage in risky behaviours such as smoking and alcohol consumption.
Exploring Bolivia: Advantages of Living in This Country
You may want to see also
Explore related products






![]()
Altitude
Bolivia's high altitude is a significant factor in the development of heart disease in the country. La Paz, Bolivia, is located 3,600 meters above sea level, where the atmosphere has lower oxygen levels than most parts of the world. This low oxygen level, or hypoxia, is the likely cause of irregular blood flow, which can lead to congenital heart defects such as Patent Ductus Arteriosus (PDA).
The reduced oxygen availability at high altitudes places additional stress on the heart and lungs, especially for those with cardiovascular disease. The heart requires more oxygen-rich blood, even at rest, and activities such as skiing, hiking, or climbing can place too much stress on the heart and blood vessels due to lower oxygen levels and fluctuations in air pressure, temperature, and humidity.
People who live at high altitudes face fewer risks as their bodies have had time to adjust to living with less oxygen. However, for those with heart conditions, it is recommended to increase altitude gradually, drink lots of fluids, limit alcohol consumption, and plan for emergencies.
Women in La Paz, Bolivia: Census Insights
You may want to see also
Explore related products






![]()
Genetics
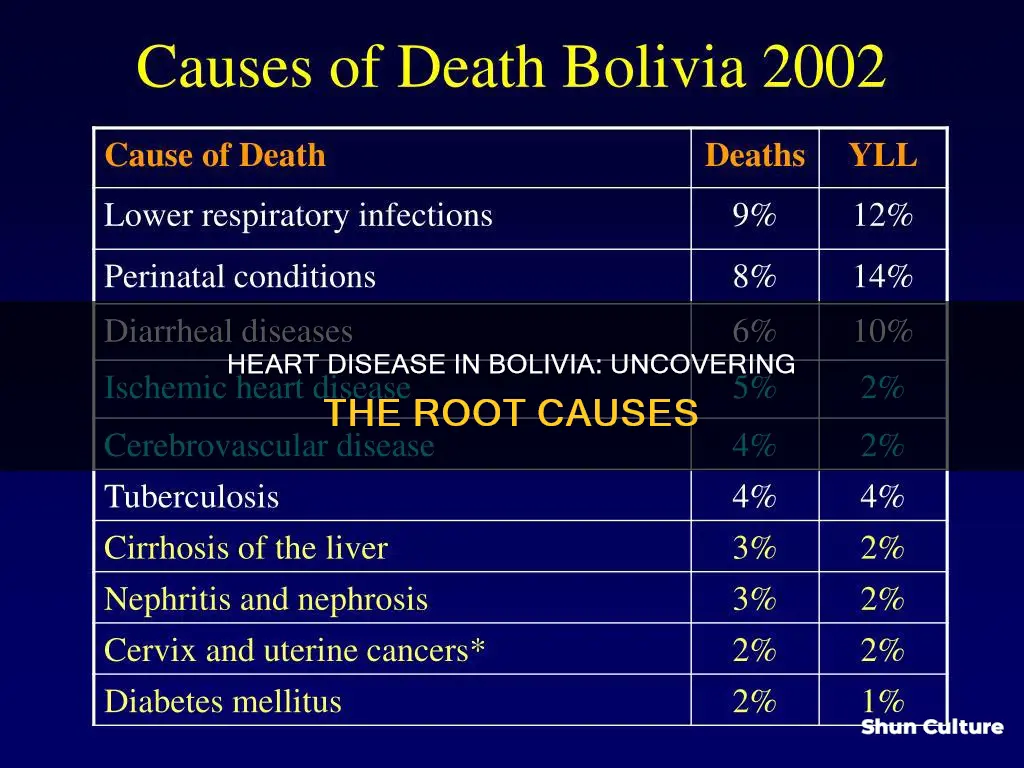
In Bolivia, the Pan American Health Organization (PAHO) has reported that non-communicable diseases (NCDs) are responsible for 59% of overall mortality, with cardiovascular diseases (CVDs) accounting for 24% of total deaths. However, these statistics are only estimates, and more accurate data is needed to inform public health interventions.
A 2019 study in Cochabamba, Bolivia, found that the prevalence of behavioural risk factors for CVDs was as follows:
- Current smoking: 11.6%
- Current alcohol consumption: 42.76%
- Low consumption of fruits and vegetables: 76.73%
- Low level of physical activity: 64.77%
- Overweight: 35.84%
- Obesity: 20.49%
- Abdominal obesity: 54.13%
- Raised blood pressure: 17.5%
The study also revealed that indigenous populations and those living in the Andean region generally had a lower prevalence of most risk factors. Additionally, men, individuals living in the tropics area, and workers were found to have a significantly higher risk of smoking and alcohol consumption.
While genetics may play a role in heart disease, the evidence suggests that lifestyle and environmental factors are more influential in Bolivia. Addressing these modifiable risk factors through public health interventions and education can help reduce the burden of CVDs in the country.
Exploring Bolivia: Discovering Its Vibrant Urban Centers
You may want to see also
Explore related products

$171.7





![]()
Poverty
Bolivia is the second poorest country in South America, with a poor performance in education, life expectancy, economic strength and overall development. The country also lacks sufficient medical care due to a limited supply of resources. This lack of healthcare access is a significant factor in the high prevalence of cardiovascular disease (CVD) in Bolivia.
CVD is the number one cause of death worldwide, especially in low- and middle-income countries, including Bolivia. In 2015, 80% of global deaths from CVD were in low to middle-income countries. The World Health Organization reports that 37% of premature deaths in these countries are caused by CVD.
In Bolivia, non-communicable diseases are responsible for 59% of overall mortality, with CVD alone causing 24% of total deaths. However, these figures are only estimates, and more accurate information is needed to support decision-making. The lack of accurate information about CVD prevalence and associated risk factors is one of the major difficulties in implementing preventive local health programs in the country.
The prevalence of CVD risk factors in Bolivia is high. A study in Cochabamba, Bolivia, found that 11.6% of participants were current smokers, 42.76% were consuming alcohol, 76.73% had a low consumption of fruits and vegetables, and 64.77% had a low level of physical activity. Additionally, 35.84% were overweight, 20.49% were obese, 54.13% had abdominal obesity, and 17.5% had raised blood pressure.
The high prevalence of CVD risk factors in Bolivia can be attributed in part to poverty. Poverty can lead to limited access to healthcare, unhealthy diets, and a lack of physical activity, all of which are risk factors for CVD. Additionally, poverty can make it difficult for individuals to afford healthy foods, such as fruits and vegetables, which are often more expensive than processed or fast food. Poverty can also contribute to stress and unhealthy coping mechanisms, such as smoking and alcohol consumption, which are also risk factors for CVD.
The effects of poverty on CVD are further compounded by the lack of diagnostic tools and affordable medications for CVD in low- and middle-income countries. This can result in delayed diagnoses and limited access to treatment, leading to increased mortality from CVD.
Addressing the underlying social and economic determinants of health, such as poverty, is crucial to reducing the burden of CVD in countries like Bolivia. This includes improving access to healthcare, promoting healthy diets and physical activity, and addressing the social and economic factors that contribute to unhealthy behaviours.
Exploring the Rich Cultural Diversity of Bolivia's Nationality
You may want to see also
Frequently asked questions
According to a study conducted in Cochabamba, Bolivia, the prevalence of behavioural risk factors for cardiovascular disease (CVD) were: current smoking (11.6%), current alcohol consumption (42.76%), low consumption of fruits and vegetables (76.73%), and low levels of physical activity (64.77%). Other risk factors included being overweight (35.84%), obesity (20.49%), abdominal obesity (54.13%), and raised blood pressure (17.5%).
Bolivia's unique geography poses challenges for accessing adequate medical care, especially for those living in rural areas. Additionally, the high altitude of certain regions, such as La Paz, can contribute to decreased oxygen levels, which can impact fetal heart health and increase the risk of congenital heart defects.
The Tsimane people have been found to have the healthiest hearts in the world, with very low rates of heart disease and hardening of the arteries. Their lifestyle involves subsistence farming, foraging, and physical activity, with men engaging in hunting and fishing while women work on farms and tend to children. This results in an active lifestyle, with men averaging 17,000 steps per day and women averaging 16,000 steps per day. Their diet is primarily plant-based, consisting of non-processed carbohydrates such as rice, plantains, corn, nuts, and fruits, with protein sourced from lean wild game and fish.
The main causes of heart disease in Bolivia are multifaceted and can include behavioural risk factors such as smoking, alcohol consumption, physical inactivity, and dietary choices. Additionally, socioeconomic factors, such as limited access to healthcare and low income, can also contribute to the prevalence of heart disease in the country.
Congenital heart defects, such as Patent Ductus Arteriosus (PDA), are a significant issue in Bolivia, particularly in certain regions like La Paz. Franz Freudenthal, an inventor and cardiologist, has developed a simple technique called the Nit Occlud device, which utilizes an indigenous knitting technique to create a heart-closure device. This innovation has saved the lives of over 2,500 children in nearly 60 countries, including Bolivia.