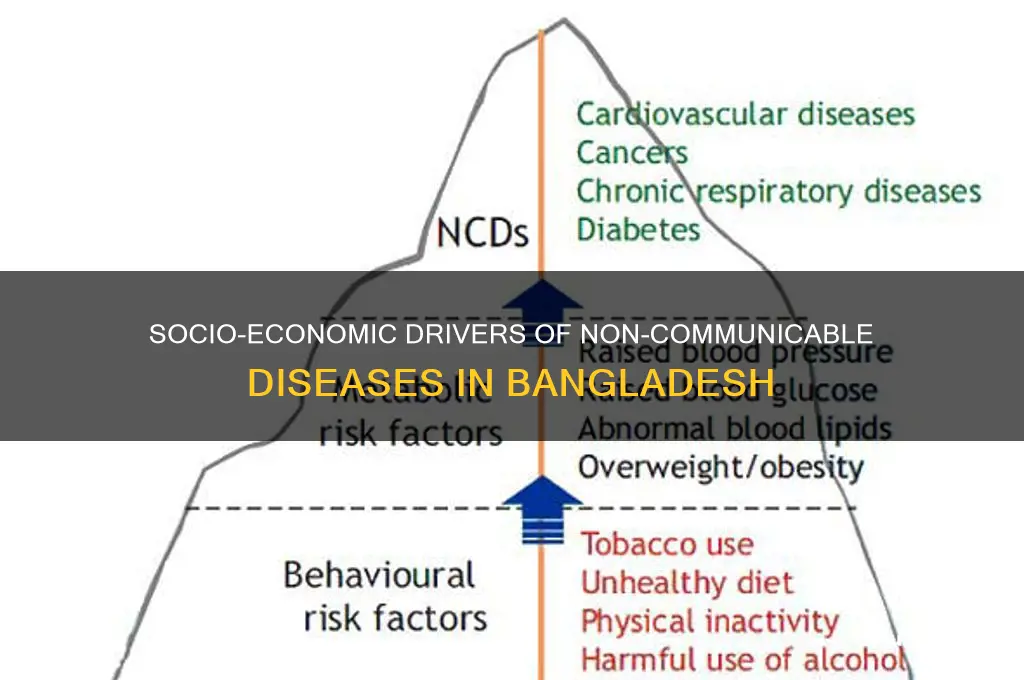
Non-communicable diseases (NCDs) such as cardiovascular diseases, diabetes, cancer, and chronic respiratory diseases have emerged as a significant public health challenge in Bangladesh, accounting for a growing proportion of morbidity and mortality. The socio-economic factors contributing to the rise of NCDs in the country are multifaceted, encompassing rapid urbanization, changing lifestyles, and increasing consumption of unhealthy diets. Poverty and income inequality exacerbate the situation, limiting access to healthcare services and health education, particularly in rural and marginalized communities. Additionally, the prevalence of tobacco use, physical inactivity, and occupational hazards further compounds the risk of NCDs. Understanding these socio-economic determinants is crucial for developing targeted interventions and policies to mitigate the burden of NCDs and promote healthier outcomes for the Bangladeshi population.
Explore related products





What You'll Learn
- Urbanization and lifestyle changes impact NCD prevalence in Bangladesh's growing cities
- Poverty links to limited healthcare access, increasing NCD risks among low-income groups
- Tobacco and unhealthy diets contribute significantly to NCDs in Bangladeshi populations
- Education levels influence awareness and prevention of non-communicable diseases nationwide
- Workplace stress and long hours exacerbate NCD incidence in Bangladesh's labor force
![]()
Urbanization and lifestyle changes impact NCD prevalence in Bangladesh's growing cities
Bangladesh's rapid urbanization has transformed its landscape, with cities like Dhaka and Chittagong experiencing explosive population growth. This shift from rural to urban living brings a unique set of challenges, particularly in the realm of health. Non-communicable diseases (NCDs) such as diabetes, cardiovascular diseases, and cancer are on the rise, and urbanization plays a significant role in this trend. The urban environment, characterized by high population density, limited green spaces, and increased pollution, contributes to a sedentary lifestyle and unhealthy dietary habits, both of which are major risk factors for NCDs.
Consider the daily routine of an urban dweller in Bangladesh. Long commutes, often in congested traffic, leave little time for physical activity. The availability of processed and fast foods, coupled with a decline in traditional, nutrient-rich diets, further exacerbates the problem. For instance, a study found that urban residents in Bangladesh consume significantly higher amounts of sugar and saturated fats compared to their rural counterparts. This dietary shift, combined with reduced physical activity, leads to obesity, a key risk factor for NCDs. The World Health Organization (WHO) reports that the prevalence of obesity in urban areas of Bangladesh has increased by 20% over the past decade, with the highest rates observed among adults aged 35-55.
To mitigate these risks, urban planning and policy interventions are essential. Cities can promote healthier lifestyles by developing pedestrian-friendly infrastructure, such as sidewalks and bike lanes, and by creating accessible green spaces for recreational activities. For example, the Dhaka South City Corporation has initiated a program to establish community parks and fitness zones in densely populated areas. Additionally, public health campaigns can raise awareness about the importance of a balanced diet and regular exercise. Practical tips include incorporating at least 30 minutes of moderate-intensity physical activity daily, such as brisk walking or cycling, and reducing sugar intake to less than 10% of total energy consumption, as recommended by the WHO.
A comparative analysis of urban and rural health outcomes highlights the urgency of addressing these issues. While rural areas still face challenges related to infectious diseases and limited healthcare access, urban areas are increasingly burdened by NCDs. This disparity underscores the need for targeted interventions that account for the unique socio-economic context of Bangladesh's growing cities. By fostering healthier urban environments and empowering individuals to make informed lifestyle choices, Bangladesh can curb the rising tide of NCDs and improve overall public health.
In conclusion, the interplay between urbanization and lifestyle changes is a critical driver of NCD prevalence in Bangladesh's cities. Addressing this issue requires a multi-faceted approach, combining urban planning, public health initiatives, and individual behavioral changes. As Bangladesh continues to urbanize, prioritizing health in the design and development of its cities will be paramount to ensuring a healthier future for its urban population.
Does Newegg Ship to Bangladesh? A Comprehensive Guide for Buyers
You may want to see also
Explore related products






![]()
Poverty links to limited healthcare access, increasing NCD risks among low-income groups
In Bangladesh, poverty serves as a critical barrier to healthcare access, disproportionately exposing low-income groups to heightened risks of non-communicable diseases (NCDs). For instance, a 2020 study revealed that only 34% of the poorest quintile in Bangladesh had access to essential healthcare services, compared to 67% of the wealthiest quintile. This disparity underscores how financial constraints limit preventive care, early diagnosis, and consistent treatment, all of which are vital for managing NCDs like diabetes, hypertension, and cardiovascular diseases. Without these interventions, minor health issues often escalate into chronic conditions, creating a cycle of illness and economic hardship.
Consider the case of rural households, where nearly 70% of out-of-pocket health expenditures push families further into poverty. For a family earning less than $2 per day, the cost of a single doctor’s visit or a month’s supply of hypertension medication (averaging $10–$15) is unaffordable. This financial burden forces many to forgo treatment altogether or rely on substandard alternatives, such as purchasing cheaper, unregulated medicines from local shops. Such practices not only worsen health outcomes but also increase the likelihood of complications, which require even costlier interventions later.
The link between poverty and NCD risks is further exacerbated by limited health literacy and infrastructure in low-income areas. In urban slums and rural villages, where 80% of the population lacks access to nearby health facilities, individuals often delay seeking care until symptoms become severe. For example, a 2019 survey found that only 15% of low-income respondents with diabetes in Bangladesh were aware of their condition before experiencing acute complications. This delay in diagnosis and treatment is directly tied to the scarcity of affordable screening programs and the absence of community health workers trained in NCD management.
To break this cycle, targeted interventions are essential. One practical step is to expand community-based health programs that offer free or subsidized screenings for NCD risk factors, such as blood pressure and glucose levels. For instance, mobile health clinics could be deployed in underserved areas, providing on-the-spot tests and referrals. Additionally, subsidizing essential NCD medications through public health initiatives could reduce out-of-pocket costs, making treatment more accessible. For example, a pilot program in Bangladesh that provided free antihypertensive drugs to low-income patients saw a 40% increase in adherence rates within six months.
Ultimately, addressing the poverty-NCD nexus requires a multi-faceted approach that combines financial protection, health education, and infrastructure development. By prioritizing equitable access to healthcare, Bangladesh can mitigate the disproportionate burden of NCDs on its poorest citizens, fostering healthier and more economically resilient communities. Without such measures, the gap between the health outcomes of the rich and the poor will continue to widen, perpetuating cycles of poverty and disease.
Earn from Home in Bangladesh: Top Strategies for Steady Income
You may want to see also
Explore related products





![]()
Tobacco and unhealthy diets contribute significantly to NCDs in Bangladeshi populations
In Bangladesh, tobacco use and unhealthy dietary habits are major drivers of non-communicable diseases (NCDs), accounting for a significant portion of the country's disease burden. Tobacco consumption, particularly smoking, is alarmingly prevalent, with approximately 35% of adult males and 1.2% of adult females using tobacco products regularly. This high usage rate contributes to a range of NCDs, including cardiovascular diseases, chronic respiratory diseases, and various cancers. For instance, smoking is responsible for about 90% of lung cancer cases globally, and Bangladesh is no exception, with lung cancer being one of the leading causes of cancer-related deaths in the country.
Unhealthy diets, characterized by high intake of processed foods, sugary beverages, and low consumption of fruits and vegetables, further exacerbate the NCD crisis. A study published in the *Bangladesh Medical Research Council Bulletin* revealed that only 24% of the population consumes the recommended five servings of fruits and vegetables daily. This dietary deficiency, coupled with increasing urbanization and the availability of cheap, nutrient-poor foods, has led to a rise in obesity and related NCDs such as type 2 diabetes and hypertension. For example, the prevalence of diabetes in Bangladesh has more than tripled in the last two decades, affecting over 8% of the adult population.
Addressing these issues requires targeted interventions. For tobacco control, implementing stricter regulations on tobacco advertising, increasing taxes on tobacco products, and promoting smoking cessation programs can significantly reduce consumption. A 10% increase in tobacco taxes, for instance, has been shown to decrease consumption by 4% in low- and middle-income countries. Similarly, public health campaigns highlighting the dangers of smoking, especially among youth, can prevent initiation. For dietary improvements, subsidizing fruits and vegetables, mandating clear nutrition labels on packaged foods, and restricting the marketing of unhealthy foods to children are effective strategies. Schools and workplaces can also play a role by offering healthier meal options and educating individuals on balanced diets.
Comparatively, countries like Thailand and Mexico have successfully reduced NCDs through comprehensive policies targeting tobacco and diet. Bangladesh can draw lessons from these examples by integrating similar measures into its national health strategy. For instance, Thailand’s health-promoting school program, which includes nutrition education and physical activity, has shown measurable improvements in children’s health outcomes. By adopting such evidence-based approaches, Bangladesh can mitigate the socio-economic impact of NCDs and improve public health outcomes.
Ultimately, the interplay between tobacco use, unhealthy diets, and NCDs in Bangladesh underscores the need for urgent, multi-sectoral action. While individual behavior change is crucial, systemic interventions—such as policy reforms, economic incentives, and community engagement—are equally vital. By prioritizing these factors, Bangladesh can reduce the burden of NCDs, enhance productivity, and foster a healthier, more resilient population. Practical steps, such as limiting daily salt intake to less than 5 grams or quitting smoking through nicotine replacement therapy, can empower individuals to take control of their health while broader policies create an enabling environment for long-term change.
Understanding Bangladesh's ORTP vs IGW: Key Differences Explained
You may want to see also
Explore related products






![]()
Education levels influence awareness and prevention of non-communicable diseases nationwide
In Bangladesh, where non-communicable diseases (NCDs) like diabetes, hypertension, and cardiovascular diseases are on the rise, education levels play a pivotal role in shaping awareness and preventive behaviors. Studies show that individuals with higher education are more likely to understand health risks, adopt healthier lifestyles, and seek timely medical interventions. For instance, a 2020 survey revealed that only 30% of rural Bangladeshis with primary education could identify symptoms of hypertension, compared to 70% of those with secondary or higher education. This disparity underscores how education acts as a critical determinant in combating NCDs.
Consider the practical implications of education on preventive measures. Educated individuals are more likely to follow medical advice, such as adhering to prescribed dosages of medications like metformin (500–1000 mg daily for diabetes management) or maintaining a low-sodium diet to control blood pressure. They are also better equipped to interpret health information, such as understanding the importance of regular check-ups for adults over 40, a high-risk age group for NCDs. In contrast, low literacy rates in certain regions, particularly among women and older adults, hinder access to life-saving knowledge, perpetuating unhealthy habits like tobacco use or excessive oil consumption in cooking.
To bridge this gap, targeted interventions are essential. For example, community health workers can conduct workshops in local languages, focusing on age-specific risks and actionable steps. For adolescents, this might include promoting physical activity (at least 60 minutes daily) and limiting sugary beverages. For middle-aged adults, emphasis should be on stress management techniques and early detection of conditions like prediabetes. Pairing these efforts with visual aids and simple messaging ensures that even those with limited education can grasp key concepts, fostering a culture of prevention nationwide.
The persuasive power of education extends beyond individual behavior to policy influence. Educated populations are more likely to demand better healthcare infrastructure, such as accessible screening facilities and affordable medications. In Bangladesh, where out-of-pocket expenses for NCD treatment can push families into poverty, educated communities can advocate for subsidies on essential drugs like statins or insulin. This collective action not only reduces disease burden but also alleviates the socio-economic strain on families, creating a ripple effect of positive change.
Ultimately, investing in education is a long-term strategy to curb the NCD epidemic in Bangladesh. By integrating health literacy into school curricula, from primary to tertiary levels, the nation can cultivate a generation aware of the risks and empowered to act. For instance, teaching children about the dangers of smoking or the benefits of a balanced diet can prevent habits that lead to chronic diseases later in life. As education levels rise, so too will the nation’s capacity to tackle NCDs, transforming awareness into actionable prevention and healthier futures.
Understanding the Root Causes of Bangladesh's Water Scarcity Crisis
You may want to see also
Explore related products






![]()
Workplace stress and long hours exacerbate NCD incidence in Bangladesh's labor force
Bangladesh's labor force is increasingly burdened by non-communicable diseases (NCDs), with workplace stress and long hours emerging as significant contributors. A 2021 study published in the *Journal of Occupational Health* found that Bangladeshi garment workers, who often work 12-14 hour shifts, six days a week, reported higher levels of hypertension and diabetes compared to the general population. This correlation underscores the direct link between grueling work conditions and the rise of NCDs.
The mechanism is clear: prolonged stress triggers the release of cortisol, a hormone that, in excess, can lead to insulin resistance, elevated blood pressure, and inflammation—all precursors to NCDs. For instance, a 2019 survey by the Bangladesh Institute of Labour Studies revealed that 60% of factory workers in Dhaka exhibited symptoms of chronic stress, with 35% showing early signs of cardiovascular disease. These statistics highlight the urgent need for interventions targeting workplace environments.
To mitigate this crisis, employers must adopt evidence-based strategies. Implementing mandatory 30-minute breaks every 4 hours, as recommended by the World Health Organization, can reduce stress-related health risks. Additionally, providing access to mental health resources, such as counseling services, and promoting physical activity through on-site gyms or yoga sessions can significantly improve worker well-being. For example, a pilot program in Chittagong’s shipbuilding industry saw a 25% reduction in stress-related absenteeism after introducing these measures.
However, policy changes alone are insufficient. Workers must also be empowered to advocate for their health. Educating employees about the early signs of NCDs—such as persistent fatigue, unexplained weight gain, or frequent headaches—can lead to earlier diagnoses and treatment. Furthermore, labor unions should negotiate for stricter regulations on working hours, ensuring no employee exceeds 50 hours per week, a threshold beyond which health risks spike dramatically.
In conclusion, addressing workplace stress and long hours is not just a moral imperative but a public health necessity. By combining employer initiatives, policy reforms, and worker education, Bangladesh can curb the growing incidence of NCDs in its labor force, fostering a healthier and more productive workforce.
Mastering German in Bangladesh: Effective Strategies for Language Learners
You may want to see also
Frequently asked questions
The key socio-economic factors include rapid urbanization, leading to sedentary lifestyles and unhealthy diets; increasing income disparities, which limit access to healthcare and nutritious food for the poor; and low health literacy, resulting in inadequate awareness about NCD prevention.
Poverty exacerbates NCDs by limiting access to affordable healthcare, nutritious food, and preventive services. Poor individuals often rely on cheap, processed foods high in sugar, salt, and fat, increasing their risk of NCDs like diabetes and hypertension.
Education plays a critical role in raising awareness about healthy lifestyles, early detection, and management of NCDs. Higher education levels are associated with better health-seeking behavior, reduced risk factors, and improved adherence to treatment regimens.