Bangladesh has made significant strides in addressing HIV/AIDS, but the epidemic remains a public health concern, albeit at a low prevalence rate. As of recent estimates, the country has approximately 10,000 people living with HIV, with new infections primarily concentrated among key populations such as sex workers, men who have sex with men, and injecting drug users. Despite these numbers, Bangladesh’s overall HIV prevalence remains below 0.1%, reflecting the success of prevention and awareness programs. However, challenges persist, including stigma, limited access to testing, and inadequate healthcare infrastructure, particularly in rural areas. Continued efforts are essential to sustain progress, improve detection, and ensure access to antiretroviral therapy for those affected.
Explore related products

$61.04 $79.99





What You'll Learn
![]()
HIV prevalence trends in Bangladesh
HIV prevalence in Bangladesh has historically remained relatively low compared to other countries in South and Southeast Asia, but the trend has shown subtle shifts over the past two decades. According to the Joint United Nations Programme on HIV/AIDS (UNAIDS) and the National AIDS/STD Programme (NASP) of Bangladesh, the estimated number of people living with HIV (PLHIV) in the country has gradually increased from around 7,000 in 2005 to approximately 15,000 in 2021. This rise, while modest, reflects both improved detection methods and ongoing challenges in prevention and awareness. The prevalence rate among the general population remains below 0.1%, but specific high-risk groups, such as injecting drug users, male sex workers, and hijra (transgender) communities, exhibit disproportionately higher rates, underscoring the concentrated nature of the epidemic in Bangladesh.
One notable trend is the shift in the demographic and geographic distribution of HIV cases. Initially, HIV prevalence was concentrated in urban areas, particularly in Dhaka and Chittagong, due to higher population density and mobility. However, recent data indicates a gradual spread to rural areas, driven by migration, lack of awareness, and limited access to healthcare services. This trend highlights the need for decentralized HIV prevention and treatment programs to address emerging hotspots effectively. Additionally, the age group most affected has shifted slightly, with younger individuals, particularly those aged 15–24, now accounting for a larger proportion of new infections, emphasizing the importance of targeted youth-focused interventions.
Another critical trend is the role of key populations in driving HIV transmission. Injecting drug users remain the group with the highest prevalence, with rates exceeding 5% in some studies. Despite harm reduction programs, such as needle-syringe exchange and opioid substitution therapy, coverage remains inadequate, particularly outside major cities. Similarly, male sex workers and hijra communities face significant stigma and discrimination, limiting their access to testing and treatment services. These challenges are compounded by low condom use and limited knowledge about HIV prevention, contributing to sustained transmission within these groups.
On a positive note, Bangladesh has made strides in scaling up antiretroviral therapy (ART) and improving access to HIV testing. As of 2021, approximately 60% of PLHIV were aware of their status, and around 50% were receiving ART. This progress is partly due to increased funding from international donors and the government’s commitment to achieving the UNAIDS 95-95-95 targets (95% of PLHIV knowing their status, 95% on treatment, and 95% virally suppressed). However, gaps remain, particularly in reaching key populations and ensuring consistent adherence to treatment, which are essential for reducing new infections and AIDS-related deaths.
In conclusion, while HIV prevalence in Bangladesh remains low, the trends indicate a need for sustained and targeted efforts to prevent further spread. Addressing the epidemic requires a multi-pronged approach, including expanding harm reduction services, reducing stigma and discrimination, and enhancing HIV education and testing, especially among high-risk groups and in rural areas. By leveraging lessons learned and building on existing programs, Bangladesh can continue to mitigate the impact of HIV and work toward controlling the epidemic in the long term.
Free Calls to Bangladesh: Easy Methods to Stay Connected
You may want to see also
Explore related products






![]()
High-risk groups and HIV rates
As of the latest available data, Bangladesh has a relatively low HIV prevalence rate compared to other countries in the region, with an estimated 7,500 people living with HIV (PLHIV) as of 2021. However, the epidemic is concentrated among specific high-risk groups, and understanding these groups is crucial for targeted intervention and prevention strategies. The primary high-risk populations in Bangladesh include injecting drug users (IDUs), male and female sex workers, men who have sex with men (MSM), transgender individuals, and hijra communities. These groups face a disproportionately higher risk of HIV infection due to behavioral, social, and structural factors.
Injecting Drug Users (IDUs) are among the most vulnerable populations, with an estimated HIV prevalence rate of 3.5% as per recent studies. The sharing of contaminated needles and syringes among IDUs significantly contributes to the spread of HIV. Additionally, the stigma and criminalization of drug use often prevent this group from accessing harm reduction services, such as needle-syringe programs and opioid substitution therapy, which are essential for reducing HIV transmission.
Sex workers, both male and female, also face elevated HIV risks, with prevalence rates ranging from 1% to 2%. Female sex workers (FSWs) are particularly vulnerable due to inconsistent condom use, multiple partnerships, and limited access to healthcare services. Male sex workers and MSM, including those who sell sex to other men, have an even higher HIV prevalence, estimated at around 5%. This is attributed to high-risk sexual behaviors, social marginalization, and a lack of tailored HIV prevention programs for these communities.
Transgender individuals and hijras (a traditional third-gender community in South Asia) are another high-risk group, with HIV prevalence rates as high as 8% in some studies. These communities often face severe discrimination, violence, and exclusion from healthcare and social services, forcing many into sex work for survival. The intersection of stigma, poverty, and limited access to HIV testing and treatment exacerbates their vulnerability to HIV infection.
Despite the concentrated nature of the epidemic, Bangladesh has made progress in scaling up HIV prevention and treatment services for these high-risk groups. Programs such as the National AIDS/STD Program (NASP) focus on providing targeted interventions, including condom distribution, behavioral change communication, and antiretroviral therapy (ART) for PLHIV. However, challenges remain, including inadequate funding, limited coverage of interventions, and persistent social stigma against these marginalized populations. Strengthening community-led initiatives and ensuring human rights-based approaches are essential to effectively address HIV among high-risk groups in Bangladesh.
Exploring Bangladesh's Berry Scene: Strawberries vs. Blueberries - Which Grows?
You may want to see also
Explore related products






![]()
Regional HIV distribution in Bangladesh
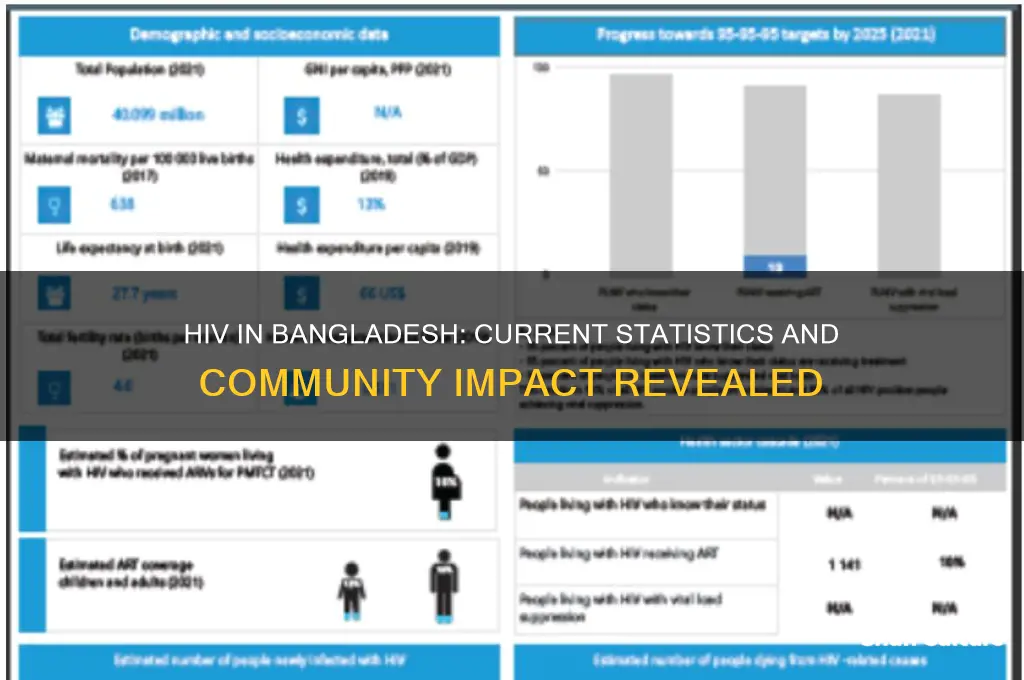
As of recent data, Bangladesh has a relatively low HIV prevalence rate compared to other countries in South Asia, with an estimated 7,500 people living with HIV (PLHIV) as of 2021. However, the distribution of HIV cases across different regions in Bangladesh is not uniform, and certain areas report higher concentrations of infections. Understanding the regional distribution is crucial for targeted interventions and resource allocation.
The Dhaka Division, which includes the capital city of Dhaka, is the most affected region in Bangladesh. This is largely due to its high population density, urbanization, and greater mobility of people, including migrant workers and sex workers. Dhaka Division accounts for a significant proportion of the country's HIV cases, with the city of Dhaka being a hotspot for new infections. The presence of key affected populations, such as injecting drug users (IDUs) and male clients of sex workers, further contributes to the higher prevalence in this region.
The Chittagong Division, particularly the port city of Chittagong, is another area of concern. Its strategic location as a major port city facilitates the movement of people, including migrant workers and truck drivers, who are at higher risk of HIV transmission. The division's HIV prevalence is lower than Dhaka but remains notable due to its economic and transportation significance. Coastal areas within this division also report cases linked to mobility and high-risk behaviors.
In contrast, the Rajshahi, Khulna, Barisal, Sylhet, and Rangpur Divisions report significantly lower HIV prevalence rates. These regions are predominantly rural, with less urbanization and lower population mobility. However, localized outbreaks have been reported in certain districts, often linked to specific high-risk groups such as IDUs or sex workers. For instance, Rajshahi Division has seen sporadic cases among IDUs, while Khulna Division has reported infections among migrant workers returning from abroad.
Regional disparities in HIV distribution are also influenced by access to healthcare and awareness programs. Urban areas like Dhaka and Chittagong have better access to HIV testing, antiretroviral therapy (ART), and prevention services compared to rural regions. This urban-rural divide exacerbates the concentration of cases in cities, as rural populations often face barriers to diagnosis and treatment. Additionally, stigma and discrimination in rural areas may deter individuals from seeking testing or disclosing their HIV status.
In summary, the regional distribution of HIV in Bangladesh is heavily skewed toward urban and economically active regions, particularly Dhaka and Chittagong Divisions. While rural areas report fewer cases, localized risks persist, especially among high-risk groups. Addressing these regional disparities requires tailored interventions, improved access to healthcare in rural areas, and targeted awareness campaigns to curb the spread of HIV across Bangladesh.
Understanding Bangladesh's Inflation Measurement: Methods, Metrics, and Economic Impact
You may want to see also
Explore related products


$13.39 $25




![]()
HIV testing and detection rates
One of the key issues affecting HIV testing rates in Bangladesh is the stigma associated with the virus, which often deters individuals from seeking testing and counseling services. This stigma is compounded by cultural and societal norms that discourage open discussions about sexual health and drug use. As a result, many at-risk individuals avoid testing, leading to late detection and higher transmission rates. Efforts to address this include community-based interventions, awareness campaigns, and the establishment of confidential testing centers. However, these initiatives require sustained funding and community engagement to be effective.
Detection rates are also influenced by the availability and distribution of testing facilities. Urban areas, particularly Dhaka and Chittagong, have better access to HIV testing services compared to rural regions. The government, in collaboration with NGOs and international organizations like UNAIDS and WHO, has been expanding testing services through voluntary counseling and testing (VCT) centers and integrated testing in healthcare facilities. Rapid diagnostic tests (RDTs) have been particularly useful in increasing detection rates, as they provide quick results and can be administered in non-clinical settings. Despite these advancements, the coverage remains inadequate to capture the true extent of HIV infections nationwide.
Another factor impacting detection rates is the integration of HIV testing into routine healthcare services. Prenatal testing for pregnant women has been successful in identifying cases and preventing mother-to-child transmission (MTCT). However, similar integration in other healthcare settings, such as tuberculosis (TB) clinics and sexually transmitted infection (STI) treatment centers, is still limited. Strengthening these linkages could significantly improve early detection and treatment initiation. Additionally, self-testing kits, though not widely available in Bangladesh, could be a game-changer in increasing testing rates by providing privacy and convenience.
In conclusion, while Bangladesh has made strides in improving HIV testing and detection rates, significant gaps remain. Addressing stigma, expanding access to testing in rural areas, and integrating testing into broader healthcare services are essential steps to achieve more accurate prevalence data and better management of HIV. Increased investment in awareness programs and infrastructure, coupled with community involvement, will be crucial in overcoming these challenges and ensuring that HIV-positive individuals receive timely diagnosis and care.
Bangladesh's Population Crisis: Is Overcrowding a Sustainable Reality?
You may want to see also
Explore related products





![]()
Government HIV prevention initiatives
The Government of Bangladesh has implemented a range of initiatives to prevent the spread of HIV and provide care for those living with the virus. According to recent estimates, Bangladesh has a relatively low HIV prevalence rate, with approximately 10,000 people living with HIV as of 2021. However, the government recognizes the importance of sustained efforts to prevent new infections and improve access to treatment. One of the key strategies is the National Strategic Plan for HIV/AIDS, which outlines a comprehensive approach to HIV prevention, treatment, and care. This plan is implemented through a multi-sectoral response involving various government ministries, non-governmental organizations (NGOs), and international partners.
A cornerstone of the government's HIV prevention initiatives is the promotion of awareness and education. The Ministry of Health and Family Welfare, in collaboration with NGOs and community-based organizations, conducts widespread awareness campaigns targeting high-risk populations, including sex workers, men who have sex with men (MSM), transgender individuals, and people who inject drugs (PWID). These campaigns utilize various media platforms, including television, radio, and social media, to disseminate information about HIV transmission, prevention methods, and the importance of testing. Additionally, peer educators and community health workers are trained to provide accurate information and counseling services at the grassroots level, ensuring that messages are culturally sensitive and accessible.
Another critical initiative is the expansion of HIV testing and counseling services. The government has established numerous testing centers across the country, offering free and confidential HIV testing. These centers are equipped with rapid diagnostic tests, providing results within minutes. To encourage testing, the government has implemented mobile testing units that reach remote and underserved areas. Furthermore, provider-initiated testing and counseling (PITC) are integrated into primary healthcare services, ensuring that individuals are tested for HIV as part of routine medical check-ups. This approach helps identify HIV-positive individuals early, enabling them to access treatment and prevent further transmission.
The government also focuses on harm reduction strategies to prevent HIV transmission among high-risk groups. For PWID, needle and syringe exchange programs (NSPs) have been established in major cities, providing clean injecting equipment and safe disposal services. These programs are often coupled with opioid substitution therapy (OST), which offers a safer alternative to illicit drug use. For sex workers and their clients, the distribution of condoms and promotion of their consistent use are prioritized. Condom promotion programs are implemented in brothels, hotels, and other venues, with peer educators playing a vital role in encouraging their use. These harm reduction measures aim to minimize the risk of HIV transmission within these vulnerable populations.
In addition to prevention efforts, the government ensures access to antiretroviral therapy (ART) for all HIV-positive individuals. ART is provided free of charge through designated healthcare facilities, with a focus on early initiation and adherence support. The government has also established a robust supply chain management system to ensure an uninterrupted supply of ART medications. To address stigma and discrimination, which can hinder access to services, the government conducts training programs for healthcare workers and law enforcement officials, promoting a rights-based approach to HIV care. These initiatives collectively contribute to Bangladesh's efforts to control the HIV epidemic and improve the quality of life for those affected.
How to Translate 'How Are You' in Bangladesh: A Quick Guide
You may want to see also
Frequently asked questions
As of recent estimates, Bangladesh has approximately 10,000 to 15,000 people living with HIV, though the exact number may vary due to underreporting and limited testing.
Bangladesh has a low HIV prevalence rate, estimated at less than 0.1% of the adult population, making it one of the countries with the lowest HIV burden globally.
Key affected populations in Bangladesh include injecting drug users, male and female sex workers, men who have sex with men (MSM), and transgender individuals, who face higher risks due to behavioral and structural factors.
Bangladesh has made progress in HIV prevention and treatment, with increased access to antiretroviral therapy (ART) and awareness campaigns. However, challenges remain in reaching marginalized groups and reducing stigma.
Key challenges include limited awareness, social stigma, inadequate testing facilities, and insufficient funding for comprehensive HIV/AIDS programs, particularly in rural areas.