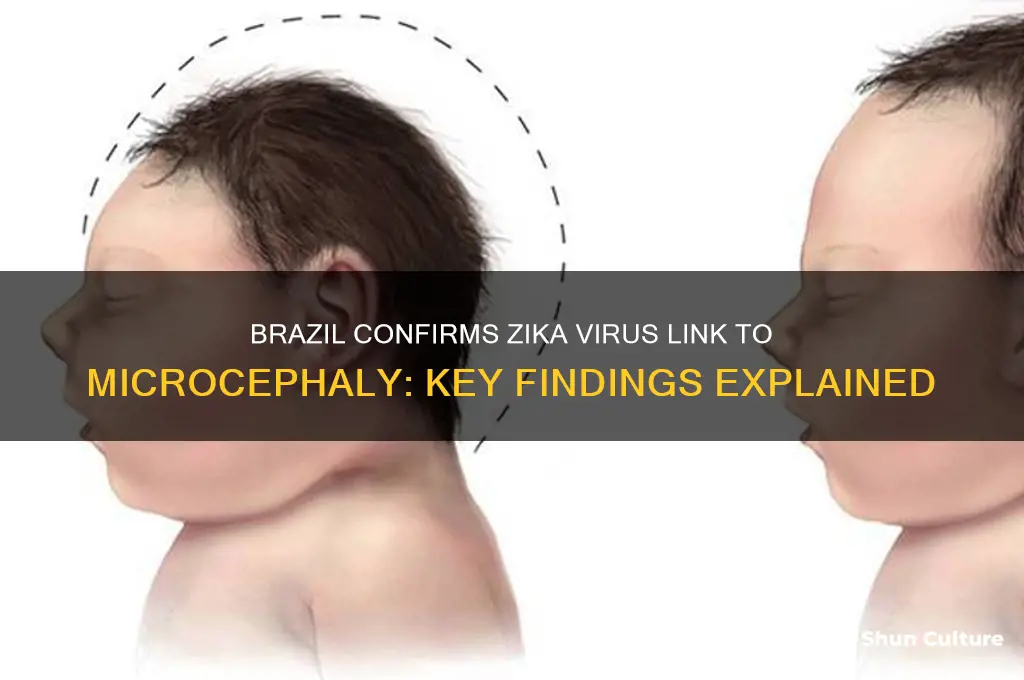
In 2015, Brazil became the epicenter of a public health crisis when a surge in cases of microcephaly, a rare birth defect characterized by an abnormally small head and potential developmental issues, coincided with the widespread outbreak of the Zika virus. As the number of affected infants grew, Brazilian health authorities launched extensive investigations to determine whether there was a causal link between Zika virus infection during pregnancy and the rise in microcephaly cases. By early 2016, after rigorous research and collaboration with international health organizations, Brazil confirmed a strong association between Zika virus and microcephaly, marking a critical turning point in global efforts to combat the virus and protect pregnant women and their unborn children.
| Characteristics | Values |
|---|---|
| Confirmation of Link | Yes, Brazil confirmed a causal relationship between Zika virus and microcephaly. |
| Year of Confirmation | 2016 |
| Evidence Basis | Epidemiological studies, case reports, and laboratory findings. |
| Key Organizations Involved | Brazilian Ministry of Health, WHO, CDC. |
| Primary Mechanism | Zika virus infection during pregnancy leading to fetal brain abnormalities. |
| Prevalence Increase | Sharp rise in microcephaly cases during the 2015-2016 Zika outbreak. |
| Geographic Impact | Most affected regions in northeastern Brazil. |
| Global Recognition | WHO declared Zika a Public Health Emergency of International Concern (PHEIC) in 2016. |
| Ongoing Research | Continued studies to understand long-term effects and improve prevention. |
| Public Health Measures | Mosquito control, travel advisories, and prenatal care guidelines. |
Explore related products




![Recombinant Zika Virus PreM Protein (Brazil) (aa 126-259) [His]](https://m.media-amazon.com/images/I/71NLoisMPDL._AC_UY218_.jpg)
What You'll Learn
- Initial Reports: Early studies suggested a correlation between Zika virus infections and microcephaly cases in Brazil
- WHO Confirmation: The World Health Organization officially confirmed the link in 2016 after extensive research?
- Epidemiological Data: Brazilian health authorities analyzed outbreak patterns to establish the Zika-microcephaly connection
- Scientific Evidence: Research identified Zika virus in fetal brain tissues, solidifying the causal relationship
- Public Health Response: Brazil implemented measures to control Zika spread and monitor microcephaly cases
![]()
Initial Reports: Early studies suggested a correlation between Zika virus infections and microcephaly cases in Brazil
In late 2015, Brazil witnessed a startling surge in microcephaly cases, a rare neurological condition causing abnormally small heads in newborns. This anomaly coincided with the rapid spread of the Zika virus, a previously mild and often asymptomatic infection. Early epidemiological studies quickly identified a temporal and geographic correlation: regions with high Zika transmission rates reported disproportionately more microcephaly cases. For instance, the state of Pernambuco, one of the hardest-hit areas, saw a 20-fold increase in microcephaly diagnoses compared to previous years. These initial observations prompted Brazilian health authorities to declare a public health emergency and investigate the potential link between Zika and microcephaly.
The first case reports emerged from northeastern Brazil, where clinicians noticed a cluster of infants born with severe microcephaly whose mothers had reported Zika-like symptoms during pregnancy. Autopsies and laboratory tests on affected fetuses and newborns detected the Zika virus in brain tissue, amniotic fluid, and placenta, providing crucial biological evidence. A 2016 study published in *The New England Journal of Medicine* analyzed data from 88 pregnant women with Zika virus infection and found that 29% of their fetuses or infants had ultrasound findings consistent with congenital infection, including microcephaly. These findings were groundbreaking, as they suggested a direct causal pathway between maternal Zika infection and fetal brain abnormalities.
However, establishing causation required more than correlation. Researchers turned to animal models to test the virus’s effects on fetal development. Experiments in pregnant mice and non-human primates exposed to the Zika virus demonstrated fetal demise, placental damage, and brain malformations, mirroring the human cases. These studies provided a mechanistic explanation: the Zika virus could cross the placental barrier, infect neural progenitor cells, and disrupt brain development. By mid-2016, the cumulative evidence from human case studies and animal experiments led the World Health Organization (WHO) and the U.S. Centers for Disease Control and Prevention (CDC) to conclude that Zika virus infection during pregnancy was a cause of microcephaly and other congenital brain abnormalities.
Despite the strength of the initial reports, challenges remained. The lack of a standardized case definition for microcephaly and the underreporting of Zika infections complicated data interpretation. Additionally, not all pregnant women infected with Zika gave birth to babies with microcephaly, indicating that other factors, such as genetic predisposition or timing of infection, might influence outcomes. For instance, first-trimester infections appeared to pose a higher risk. To address these gaps, Brazilian researchers collaborated with international teams to develop diagnostic criteria and conduct longitudinal cohort studies. By 2018, over 3,500 cases of congenital Zika syndrome had been confirmed in Brazil, solidifying the virus’s role in the microcephaly epidemic.
The initial reports from Brazil not only alerted the world to a new public health threat but also catalyzed global research efforts. They underscored the importance of real-time surveillance and interdisciplinary collaboration in emerging infectious disease outbreaks. For pregnant women in affected areas, these findings translated into practical advice: avoid mosquito bites, use condoms to prevent sexual transmission, and seek prenatal care for early detection of complications. While the Zika epidemic has subsided, its legacy endures in ongoing studies of long-term outcomes for affected children and in the development of vaccines and antiviral therapies. Brazil’s swift response and transparency in sharing data remain a model for addressing future health crises.
Brazil's Cropland Expansion: Assessing Agricultural Land Use and Impact
You may want to see also
Explore related products






![]()
WHO Confirmation: The World Health Organization officially confirmed the link in 2016 after extensive research
In 2016, the World Health Organization (WHO) made a groundbreaking announcement that reshaped global health priorities: the official confirmation of a causal link between the Zika virus and microcephaly. This declaration came after months of rigorous research, collaboration with Brazilian health authorities, and analysis of epidemiological data. The WHO’s statement was not merely a scientific finding but a call to action for countries to strengthen their public health responses, particularly in regions where Zika was rampant. This confirmation marked a turning point in the fight against the virus, providing clarity to healthcare providers, policymakers, and the public.
The WHO’s research involved dissecting Brazil’s alarming surge in microcephaly cases during the 2015-2016 Zika outbreak. Scientists examined biological samples, conducted case-control studies, and tracked the virus’s spread across affected areas. One critical piece of evidence was the detection of Zika virus RNA in the amniotic fluid of pregnant women whose fetuses showed signs of microcephaly. This finding, coupled with temporal and spatial correlations between Zika infections and birth defects, solidified the causal relationship. The WHO’s approach was meticulous, ensuring that its confirmation was based on irrefutable evidence rather than speculation.
For healthcare providers, the WHO’s confirmation meant a shift in prenatal care protocols. Pregnant women in Zika-affected areas were advised to undergo regular ultrasounds to monitor fetal development, particularly in the second trimester when microcephaly becomes detectable. Public health campaigns emphasized mosquito bite prevention, including the use of DEET-based repellents (safe for pregnant women when used as directed) and the elimination of standing water where mosquitoes breed. The WHO also recommended that couples in high-risk regions consider delaying pregnancy until the outbreak was under control.
The confirmation had far-reaching implications beyond Brazil. Countries with Aedes aegypti mosquitoes, the primary vector for Zika, were urged to ramp up surveillance and vector control measures. This included community engagement programs to educate residents about mosquito-borne diseases and the distribution of insecticide-treated bed nets in some regions. The WHO’s declaration also spurred international funding for vaccine development, with several candidates entering clinical trials shortly after. By 2023, while no Zika vaccine had been fully licensed, the groundwork laid in 2016 accelerated research and preparedness for future outbreaks.
In retrospect, the WHO’s 2016 confirmation was more than a scientific milestone—it was a testament to global collaboration in the face of a public health crisis. Brazil’s initial reports of microcephaly cases triggered a worldwide response, but it was the WHO’s definitive statement that unified efforts and mobilized resources. This episode underscores the importance of timely, evidence-based decision-making in public health, serving as a model for addressing emerging infectious diseases. For individuals and communities, the takeaway is clear: vigilance, education, and collective action are key to mitigating the impact of such threats.
Brazil's Sugar Cane Dominance: Climate, Land, and Innovation Explained
You may want to see also
Explore related products






![]()
Epidemiological Data: Brazilian health authorities analyzed outbreak patterns to establish the Zika-microcephaly connection
In late 2015, Brazil faced an unprecedented surge in microcephaly cases, a rare birth defect characterized by an abnormally small head and potential developmental issues. This alarming trend coincided with the rapid spread of the Zika virus, a previously mild mosquito-borne infection. Brazilian health authorities, recognizing the potential link, embarked on a rigorous epidemiological investigation to determine if Zika was the culprit behind the microcephaly outbreak.
Analyzing Outbreak Patterns:
Their approach involved meticulously mapping the geographical and temporal distribution of both Zika infections and microcephaly cases. They found a striking correlation: regions with the highest Zika incidence also reported the most microcephaly cases. This spatial clustering suggested a strong association between the two. Furthermore, the surge in microcephaly cases followed the Zika outbreak with a lag, consistent with the gestational period, further implicating Zika as a potential cause.
Laboratory Evidence and Case Studies:
While epidemiological data provided strong circumstantial evidence, Brazilian researchers also sought direct proof. They analyzed amniotic fluid, fetal tissue, and brain tissue from affected babies, detecting the Zika virus genome in many cases. This confirmed that the virus could cross the placenta and infect the developing fetus. Additionally, case studies of pregnant women infected with Zika during different stages of pregnancy revealed a higher risk of microcephaly when infection occurred during the first trimester.
Establishing Causality:
Establishing a definitive causal link between Zika and microcephaly required ruling out other potential factors. Brazilian authorities meticulously investigated alternative explanations, such as genetic predisposition, exposure to other pathogens, or environmental toxins. The consistent association between Zika infection and microcephaly, coupled with the absence of a plausible alternative explanation, led them to conclude that Zika was indeed the primary cause of the outbreak.
Global Impact and Ongoing Research:
Brazil's epidemiological investigation played a pivotal role in alerting the world to the dangers of Zika virus infection during pregnancy. Their findings prompted global health organizations to declare a Public Health Emergency of International Concern and spurred international research efforts. While the link between Zika and microcephaly is now well-established, ongoing research continues to explore the full spectrum of congenital Zika syndrome, which can include other severe birth defects beyond microcephaly.
Brazil Nuts and Magnesium: Uncovering the Nutritional Powerhouse Inside
You may want to see also
Explore related products






![]()
Scientific Evidence: Research identified Zika virus in fetal brain tissues, solidifying the causal relationship
The discovery of Zika virus in fetal brain tissues marked a pivotal moment in the scientific community's understanding of the virus's role in microcephaly. Researchers meticulously analyzed tissue samples from affected fetuses, employing advanced molecular techniques such as polymerase chain reaction (PCR) and immunohistochemistry. These methods allowed for the precise detection of viral RNA and proteins within the brain, providing irrefutable evidence of the virus's presence. This breakthrough not only confirmed the link between Zika and microcephaly but also shed light on the virus's ability to cross the placental barrier and directly infect fetal neural tissue.
Analyzing the implications of this finding reveals a complex interplay between viral infection and fetal development. The Zika virus targets neural progenitor cells, which are crucial for brain growth. By disrupting these cells, the virus impedes normal brain development, leading to the characteristic small head size and developmental abnormalities seen in microcephaly. Studies have shown that the timing of infection during pregnancy significantly influences the severity of outcomes, with first-trimester infections posing the highest risk. This underscores the importance of early detection and intervention in pregnant women exposed to the virus.
From a practical standpoint, healthcare providers can utilize this scientific evidence to enhance screening and management protocols. Pregnant women in Zika-endemic areas should undergo regular ultrasounds to monitor fetal head circumference and brain development. If Zika infection is suspected, amniocentesis can be performed to test for viral RNA in amniotic fluid, though this carries a small risk and should be weighed against benefits. Additionally, public health campaigns must emphasize mosquito bite prevention, including the use of EPA-approved repellents (e.g., DEET at 30% concentration for adults and 10-30% for children over 2 months) and wearing long-sleeved clothing during peak mosquito activity times.
Comparatively, the Zika outbreak highlights the challenges of emerging infectious diseases in linking causality to congenital conditions. Unlike rubella or cytomegalovirus, where causal relationships were established decades ago, Zika’s rapid spread and novel association with microcephaly required swift, collaborative research efforts. Brazil’s role in this discovery was instrumental, as the country’s high incidence of microcephaly cases during the 2015-2016 outbreak provided critical samples and data. This contrasts with regions where lower transmission rates limited sample availability, emphasizing the importance of global health surveillance in addressing such crises.
In conclusion, the identification of Zika virus in fetal brain tissues not only solidified the causal relationship with microcephaly but also transformed public health strategies. By understanding the virus’s mechanisms and risk factors, healthcare systems can better protect vulnerable populations. This evidence serves as a reminder of the power of scientific inquiry in addressing urgent health challenges and the need for continued research to combat emerging threats.
Exploring Brazilian Culture: Daily Life, Traditions, and Passions in Brazil
You may want to see also
Explore related products

![]()
Public Health Response: Brazil implemented measures to control Zika spread and monitor microcephaly cases
Brazil's public health response to the Zika outbreak was a multifaceted campaign, combining vector control, public awareness, and enhanced surveillance. At the heart of this effort was the recognition that Aedes aegypti, the mosquito vector for Zika, also transmitted dengue and chikungunya, allowing for a coordinated approach. Door-to-door campaigns educated households on eliminating standing water, the mosquito's breeding ground. This simple yet effective measure was paired with larviciding and targeted insecticide spraying in high-risk areas. For pregnant women, the most vulnerable population, the Ministry of Health issued clear guidelines: use mosquito repellent containing DEET (up to 30% concentration, applied sparingly and avoiding hands and eyes for children under 2), wear long sleeves and pants, and ensure window screens were intact.
The surveillance system for microcephaly cases underwent a rapid transformation. Brazil's Ministry of Health established a mandatory reporting system for all suspected cases, with healthcare providers required to notify authorities within 24 hours. This real-time data collection enabled rapid investigation and confirmation of cases. Specialized teams were deployed to conduct home visits, gather detailed epidemiological data, and collect biological samples for laboratory testing. The criteria for microcephaly diagnosis were standardized, ensuring consistency across the vast country. This rigorous surveillance not only tracked the spread of microcephaly but also provided crucial data for researchers working to establish the causal link between Zika and the birth defect.
A key challenge was balancing the urgency of the situation with the need for scientific rigor. While the surge in microcephaly cases strongly suggested a connection to Zika, definitive proof required time-consuming studies. Brazil's public health officials faced the difficult task of communicating this uncertainty to a frightened public. They opted for transparency, acknowledging the lack of conclusive evidence while emphasizing the precautionary principle. This approach guided their recommendations, urging pregnant women to take stringent mosquito avoidance measures without causing undue panic.
The Brazilian experience offers valuable lessons for future public health crises. First, a robust surveillance system is paramount, allowing for early detection and response. Second, vector control measures, though labor-intensive, can significantly reduce disease transmission. Third, clear and transparent communication is essential, even in the face of scientific uncertainty. Finally, the Zika outbreak highlighted the importance of international collaboration. Brazil's data and research contributed to the global understanding of the virus, ultimately leading to the World Health Organization's declaration of Zika as a Public Health Emergency of International Concern.
Exploring Brazil's Population: Size, Growth, and Demographics Unveiled
You may want to see also
Frequently asked questions
Yes, Brazil confirmed a link between the Zika virus and microcephaly in November 2015, after a significant increase in cases of the birth defect was observed in areas with Zika outbreaks.
Brazil established the connection through epidemiological studies, laboratory testing of affected infants, and the detection of the Zika virus in the amniotic fluid and brain tissue of babies with microcephaly.
Brazil first reported an unusual increase in microcephaly cases in November 2015, coinciding with the Zika virus outbreak in the country.
The WHO supported Brazil’s findings and declared the Zika virus a Public Health Emergency of International Concern in February 2016, acknowledging the causal relationship between Zika and microcephaly.
Yes, Brazil continues to conduct research to better understand the long-term effects of Zika on infants and to improve prevention and treatment strategies for microcephaly and other congenital Zika syndrome cases.



















